




| Research Article | ||
Open Vet. J.. 2026; 16(5): 2812-2822 Open Veterinary Journal, (2026), Vol. 16(5): 2812-2822 Research Article Epidemiological study of cutaneous leishmaniasis in AlgeriaLeila Bouzabata1, Mourad Zeghdoudi2*, Ahlem Chettibi3, Amel Bouzabata4 and Zihed Bouslama51Department of Biological Sciences, University of Badji Mokhtar Annaba, Annaba, Algeria 2Department of Veterinary Sciences, Chadli Bendjedid University El Tarf, El Tarf, Algeria 3Laboratory of Environmental Sciences and Agro-Ecology, Faculty of Natural and Life Sciences, Chadli Bendjedid University El Tarf, El Tarf, Algeria 4Faculty of Medicine, University of Badji Mokhtar Annaba, Annaba, Algeria 5Center of Environment Research, Annaba, Algeria *Corresponding Author: Mourad Zeghdoudi. Department of Veterinary Sciences, Chadli Bendjedid University El Tarf, El Tarf, Algeria. Email: mouradzeg [at] yahoo.fr Submitted: 27/11/2025 Revised: 27/03/2026 Accepted: 07/04/2026 Published: 31/05/2026 © 2025 Open Veterinary Journal
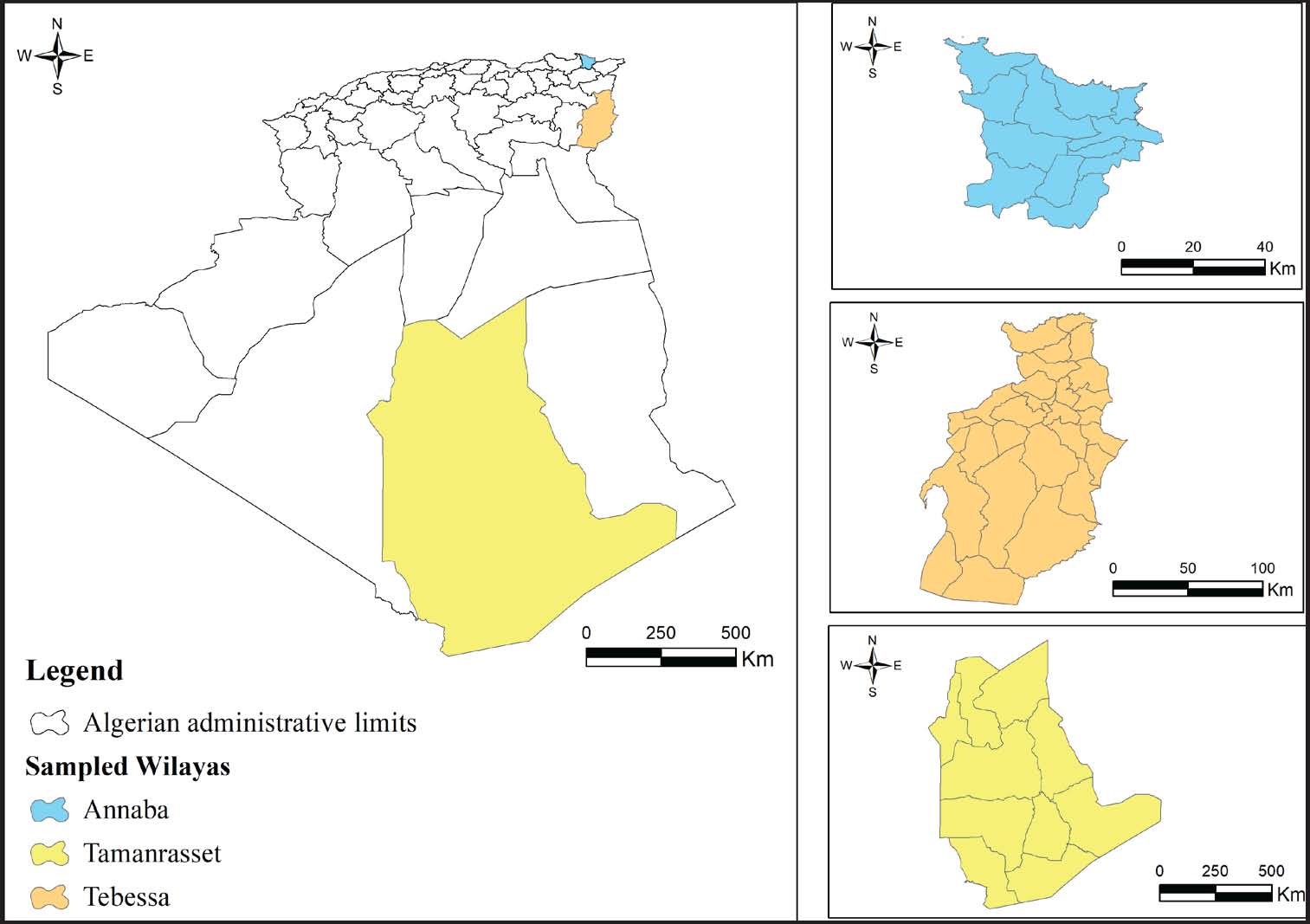
ABSTRACTBackground: Cutaneous leishmaniasis is an unstable disease characterized by unpredictable spatio-temporal fluctuations. Aim: This study aimed to identify the main risk factors involved in the persistence of this disease in Algeria. Methods: This study was conducted over 4 years in three regions of the country with different geoclimatic characteristics. The epidemiological features of the disease, its temporal dynamics during the study period, the historical background of the disease in the investigated regions, geoclimatic variations, seasonality, and sandfly abundance were investigated using statistical analyses. The investigations were conducted within the framework of an epidemiological surveillance network between 2019 and 2023. Field missions were conducted out periodically in each study region, combining active case detection in human populations with entomological surveys aimed at identifying and quantifying sandfly species. Results: Latitude and semi-arid climatic conditions have a significant impact on cutaneous leishmaniasis in Algeria. The disease’s endemic character is mainly linked to its historical presence in the affected regions, where it remains stationary. Tebessa recorded the highest mean incidence (919.2 ± 762.5), followed by Annaba (19.2 ± 14.5), whereas Tamanrasset showed the lowest (8.0 ± 5.8). A one-way ANOVA confirmed a statistically significant difference in cutaneous leishmaniasis incidence among the regions (F=7.05, p < 0.01). Conclusion: The findings indicate a stable endemic pattern of cutaneous leishmaniasis in all three regions of Algeria, with the highest incidence observed in the semi-arid region of Tebessa. This study highlighted the presence of new factors influencing the endemicity of cutaneous leishmaniasis in certain parts of the world, where effective control requires coordinated interregional or international strategies. Keywords: Cutaneous leishmaniasis, History, Latitude, Prevalence, Sandfly. IntroductionLeishmaniasis was already widespread in ancient times. The identification of the Leishmania parasite as the etiological agent and the sandfly as a transmission vector began in the early 20th century, and the discovery of new Leishmania and sandfly species has continued into the 21st century (Steverding, 2017). Leishmaniasis is a vector-borne disease caused by the flagellated protozoa of the genus Leishmania. The disease is prevalent in tropical and subtropical regions and occurs in 98 countries across Africa, Asia, Europe, and the Americas (Alvar et al., 2012). Leishmaniasis has a distinct circumterrestrial distribution, primarily intertropical, and is widespread in temperate zones of North Africa, southern Europe, and Asia. Currently, more than 90% of cases occur in only 13 countries: Afghanistan, Algeria, Tunisia, Morocco, Syria, Saudi Arabia, Egypt, India, Iran, Peru, Bolivia, Brazil, and Colombia (WHO, 2010). Leishmania is transmitted through bites of infected sandflies. Ninety-eight species belonging to the genera Phlebotomus and Lutzomyia have been described as confirmed or suspected vectors of human leishmaniasis (Maroli et al., 2013). Although different Leishmania species are morphologically very similar, they cause two main clinical forms, cutaneous leishmaniasis (CL) and visceral leishmaniasis (VL). In CL, the parasites infect resident skin macrophages. However, in VL, they infect the liver, spleen, bone marrow, lymph nodes, and intestine mononuclear phagocyte system (Steverding, 2017). The most common form is CL, with approximately 600,000 to 1 million new cases reported worldwide each year. Because there is no vaccine, drug resistance continues to emerge, and the use of new therapeutic agents remains limited, leishmaniasis is still a major public health concern. In Algeria, CL, locally known as “clou de Biskra”, was first identified in 1914 in the semi-arid zone of Biskra. Its frequency became significant only from the 2000s onward. CL is mainly caused by Leishmania major and Leishmania killicki, with rodents serving as the principal reservoirs, while Phlebotomus papatasi and Phlebotomus sergenti act as natural vectors (Garni et al., 2014). Depending on cultural, climatic, environmental, and socioeconomic factors, CL remains an unstable disease characterized by unpredictable fluctuations in case numbers. Since the epidemiology of CL remains unclear and climatic variables have become the main focus of research, this study aimed to evaluate additional risk factors associated with CL, including latitude, longitude, altitude, and historical endemicity, which, to our knowledge, have not previously been investigated in Algeria. Materials and MethodsStudy areaThis study was conducted in three distinct regions of Algeria: in the northeast, in the province of Annaba, farther south, in the locality of Tebessa, and in the region of Tamanrasset in the extreme south (Fig. 1). The city of Annaba is located in the southeastern Mediterranean area and enjoys a temperate climate with long, hot summers and mild, short winters. Humidity levels vary considerably, and rainfall is irregular. The Tebessa region, located approximately 300 km south of Annaba, is part of the vast steppe zone. The climate is continental and semi-arid, with very hot, dry summers and long, cold, and windy winters accompanied by occasional snowfall. The Tamanrasset region, located 1,900 km south of Tebessa and approximately 400 km from the Malian border, has a hot desert climate characteristic of the Hoggar massif, a mountainous massif in the heart of the Sahara. Summers are long and extremely hot, whereas winters are short and moderately warm (WorldClim, Global Climate Database).
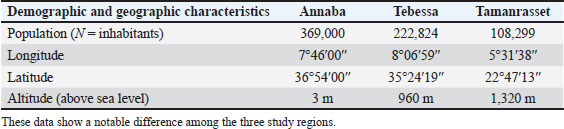
Fig. 1. Geographic location of the study areas. Geographical variablesIn the three study regions, environmental indicators such as vegetation cover were assessed using the normalized difference vegetation index (NDVI), a widely used vegetation index that provides information on changes in vegetation cover over time. NDVI data were obtained from the Copernicus Global Land Service. Bioclimatic factorsBioclimatic variables were obtained from the WorldClim global climate database (http://www.worldclim.org/current) at a spatial resolution of 1 km². Sandfly captureCDC miniature light trap (Centers for Disease Control, Atlanta, USA) was used in this study. Adhesive papers coated with castor oil were placed in areas that were less accessible to CDC traps. Sandflies were identified using standard morphological criteria based on the identification key for Algerian sandflies (Dedet et al., 1984). Statistical studyAll statistical analyses were conducted using R version 2026. The Shapiro–Wilk test was used to assess the normality of both the dependent and independent variables. To examine the relationships between CL and the various factors, we used ANOVA and Pearson’s correlation coefficient for normally distributed variables, and the Kruskal–Wallis test and Spearman’s correlation coefficient for non-normally distributed variables. A p-value < 0.05 was considered statistically significant. Multiple Correspondence Analysis (MCA) was performed to evaluate the associations among qualitative variables. Epidemiological surveillance and field investigationsThis comprehensive study was designed to identify and analyze all factors that may contribute to CL emergence and persistence in Algeria. The study focused on multiple variables, including the disease prevalence during the study period, its historical record over the previous 10 years, geoclimatic variations across the selected regions, and the abundance of sandfly vectors captured during field investigations. Each of these parameters was systematically recorded and analyzed to establish potential correlations with disease incidence using appropriate statistical methods. The investigations were conducted between 2019 and 2023 within the framework of an epidemiological surveillance network composed of local veterinary practitioners. Field missions were conducted periodically in each study region, combining active case detection in human populations with entomological surveys aimed at identifying and quantifying sandfly species. Active surveillance involved visits to local health centers and community outreach programs to document both newly diagnosed and previously recorded CL cases. The epidemiological data were cross-referenced with climatic and environmental variables obtained from national and international databases (WorldClim, meteorological stations, and NDVI). In parallel, entomological investigations were performed by installing traps (CDC miniature light traps) in strategic areas such as rural settlements, animal shelters, and peri-domestic zones known for potential vector activity. Traps were systematically placed at the beginning of each month and collected after 10 days. The traps were checked and replaced regularly to ensure representative sampling across different seasons. The collected data provide a robust foundation for assessing the temporal evolution of CL and its spatial distribution patterns. Monitoring over four consecutive years enabled the estimation of disease incidence trends and reconstruction of the epidemiological history of CL in each region since 2010. This dual approach, which combines epidemiological surveillance and environmental analysis, enabled a more comprehensive understanding of the multifactorial nature of CL transmission and persistence in Algeria. Ethical approvalThis study obtained IACUC exemption. ResultsGeographical parametersAnnaba has a typical Mediterranean climate with diverse vegetation and is located at a latitude above 36°50’. In contrast, Tebessa, situated at an intermediate latitude (35°24′), is characterized by skeletal and rocky semi-arid soils that are fragile and low in humus, where shrubs such as Artemisia are predominant. The vegetation cover is degraded and discontinuous, consisting mainly of pine, juniper, and oak. The arid zone of Tamanrasset, located at a latitude of approximately 22°, is characterized by a northern desert area and a southern rocky area with drought-resistant thorny shrubs, where the genus Acacia is dominant. Table 1 summarizes the key demographic and geographic parameters of the three study regions. Table 1. Geographical data of the three study regions.
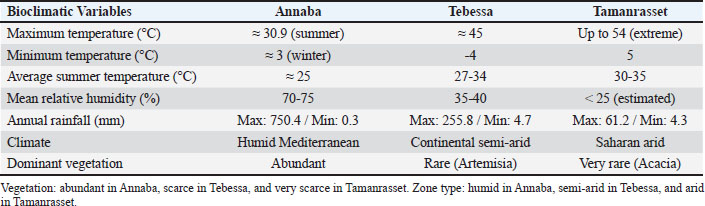
Bioclimatic variables in the study areasThe climatic characteristics of the three study regions differ markedly, reflecting Algeria’s pronounced north-south geographical gradient. Data collected between 2019 and 2023 reveal distinct temperature and humidity regimes that shape the CL transmission ecological context. Annaba, located in the humid Mediterranean zone, is characterized by moderate thermal conditions, with an average summer maximum of around 30.9°C and a mild winter minimum of close to 3°C. Relative humidity remains consistently high, generally ranging from 70% to 75%, and annual rainfall may reach up to 750 mm. These conditions support an abundant and diverse vegetation cover. Tebessa, which lies in the continental semi-arid zone, is characterized by a harsh climate and extreme temperature fluctuations. Summer temperatures often rise to 45°C, whereas winter temperatures may drop to −4°C. The region’s mean humidity is around 35–40%, and rainfall is relatively low, with annual values rarely exceeding 255 mm. The vegetation cover is sparse, dominated by resilient shrub species such as Artemisia. In contrast, Tamanrasset, which is located in the Saharan arid zone, experiences some of the highest recorded temperatures in the country, reaching up to 54°C during the hottest periods. Humidity levels are below 25%, and the average annual rainfall is less than 61 mm. Vegetation is extremely scarce, mainly drought-resistant species such as Acacia. These pronounced climatic differences (Table 2) provide an essential environmental context for understanding how temperature, humidity, and rainfall gradients across Algeria may influence the epidemiology and vector dynamics of CL. Table 2. Climatic data recorded between 2019 and 2023 (meteorological stations).
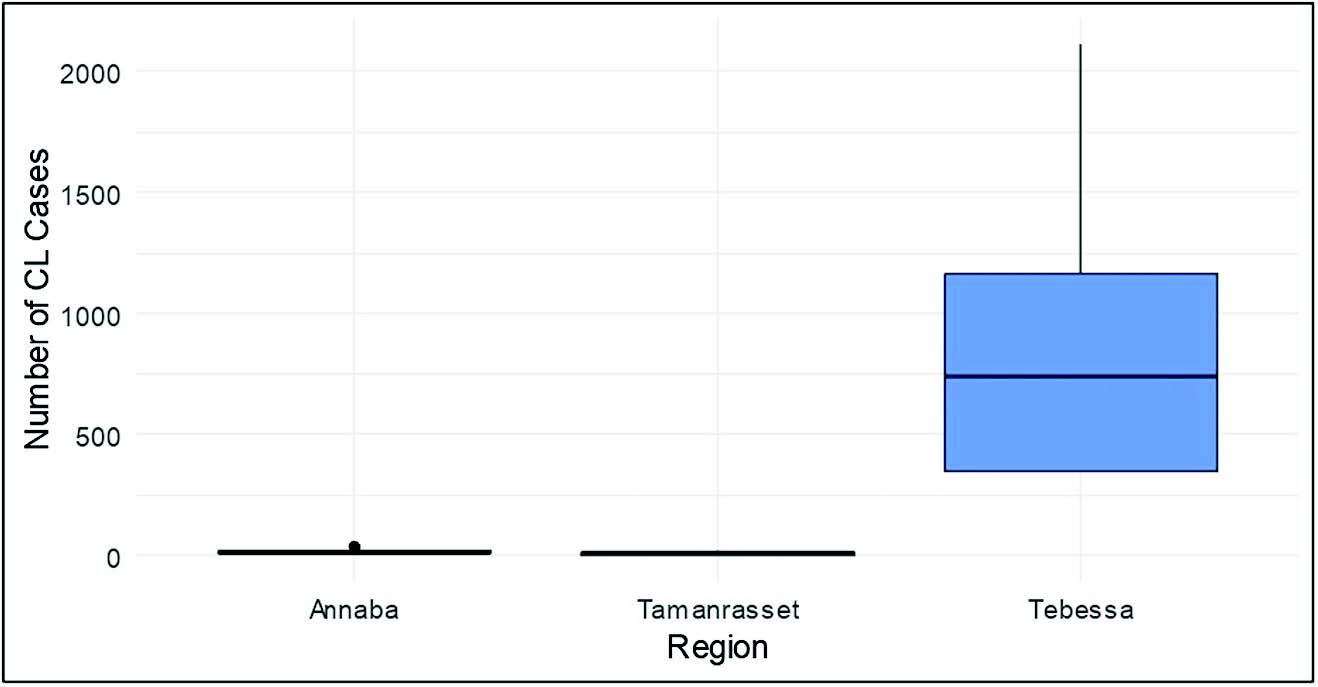
Spatiotemporal evolution and CL historical trendsCL surveillance between 2019 and 2023 revealed considerable heterogeneity among the three study regions. Tebessa recorded a total of 4,596 CL cases with the highest mean prevalence (919.2 ± 762.5), followed by Annaba, with 96 CL cases and a mean prevalence of 19.2 ± 14.5, whereas Tamanrasset reported 40 CL cases, with the lowest mean prevalence (8.0 ± 5.8). One-way ANOVA analysis of CL distribution during the study period (2019-2023) revealed a statistically significant difference between regions (F=7.05, p < 0.01). Figure 2 illustrates the spatial distribution of CL cases during the study period. In addition, Kruskal-Wallis analysis of historical CL data (2010-2018), summarized in Table 3, indicated a highly significant difference across regions (χ²=18.99, p < 0.001). Table 3. CL history in the three regions in terms of the number of cases from 2010 to 2018.
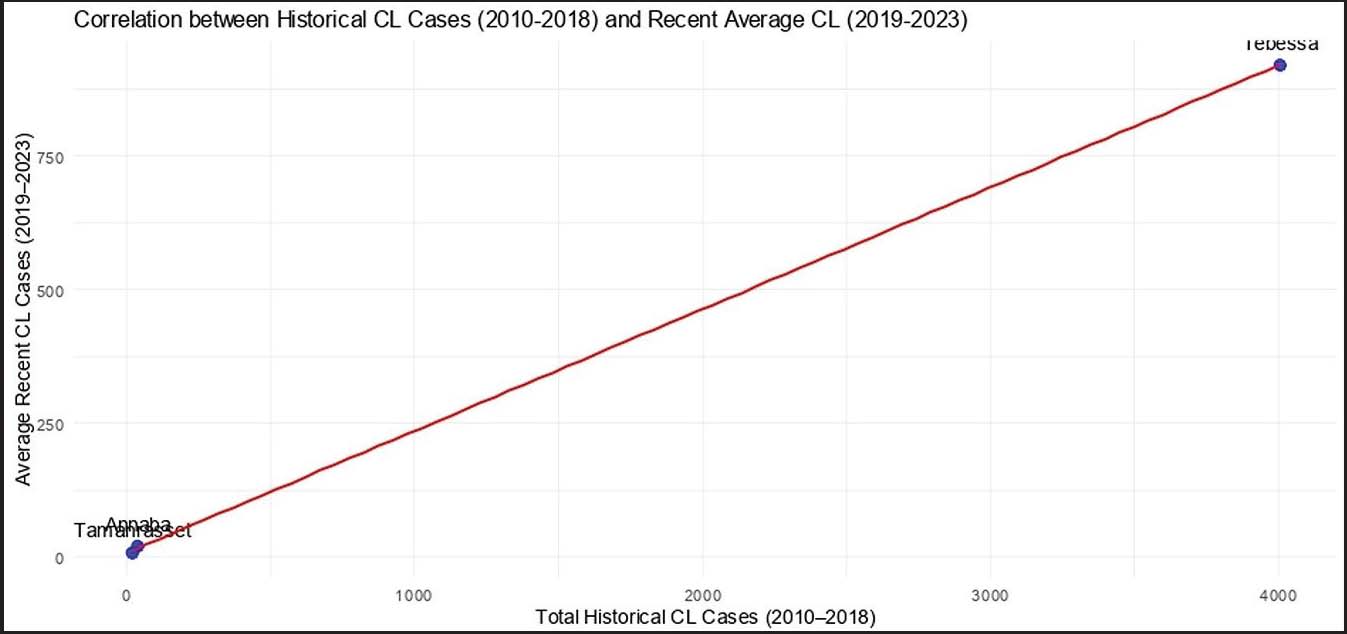
Fig. 2. Spatial distribution of CL cases across the three study regions. A strong positive correlation (r> 0.90, p< 0.05) was observed between historical and recent CL incidence (Fig. 3), indicating that regions with a long-standing history of the disease continue to report higher case numbers. A univariate logistic regression analysis was performed to further examine this relationship and assess the effect of historical CL incidence on the risk of high current CL cases. The model showed a significant association between historical cases and the likelihood of high incidence (OR=1.018; 95% CI: 1.008-1.030; p < 0.001). This result indicates that for each additional historical case, the odds of observing a high incidence in a given year increase by approximately 1.8%. Consequently, regions with a higher historical incidence are more likely to report current cases, confirming that areas with a long-standing history of CL remain at greater risk. Overall, these findings support the persistence of CL in historically endemic zones and emphasize the role of long-term environmental and socio-ecological stability in maintaining transmission. Despite environmental contrasts among “humid”, “semi-arid”, and “arid” zones, the historical morbidity burden appears to reflect underlying biological, ecological, and socioenvironmental determinants. Therefore, historical trends likely represent the persistence of these underlying factors over time.
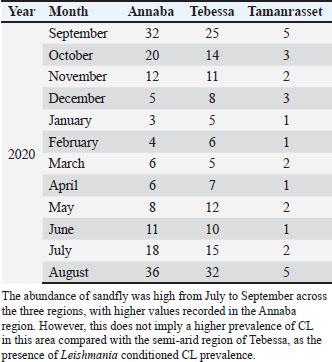
Fig. 3. Correlation between historical and current CL incidences during the study period (2019-2023). Sandfly abundanceEntomological surveillance was conducted in 2020 to better understand the spatial distribution of CL in relation to the presence and density of sandflies. The number of captured sandflies varied significantly by region and month, reflecting both climatic conditions and vector activity cycles. Table 4 shows that sandfly abundance peaked during the late summer months, particularly in August, when temperatures and humidity levels favored their proliferation. Table 4. Number of sandflies captured per month in 2020.
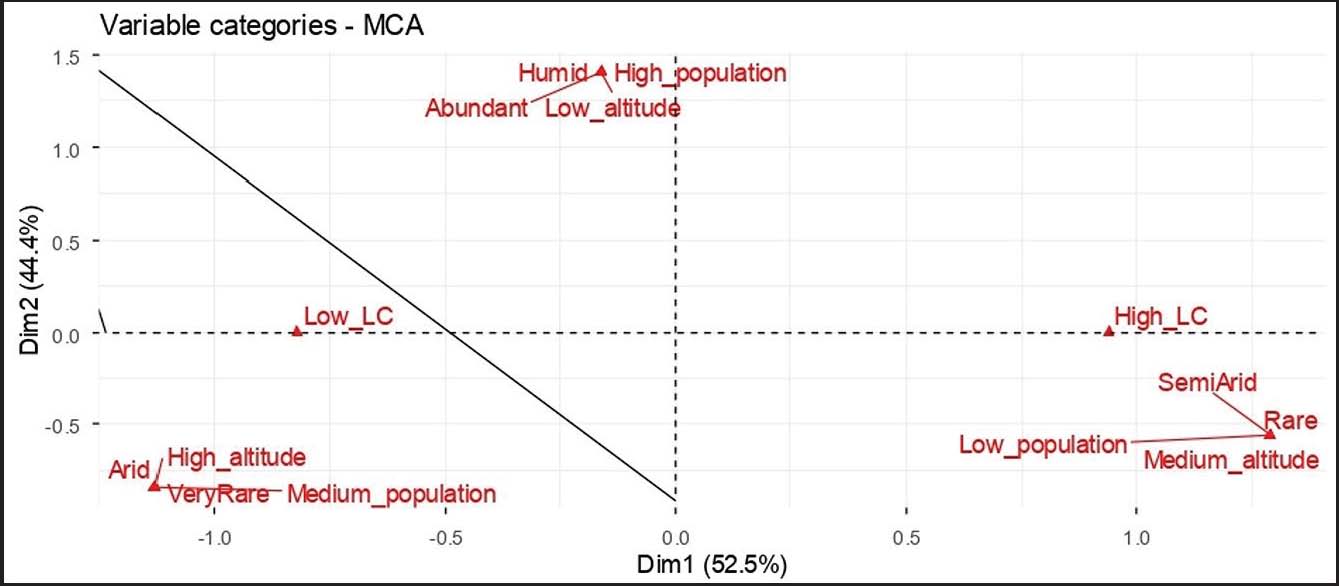
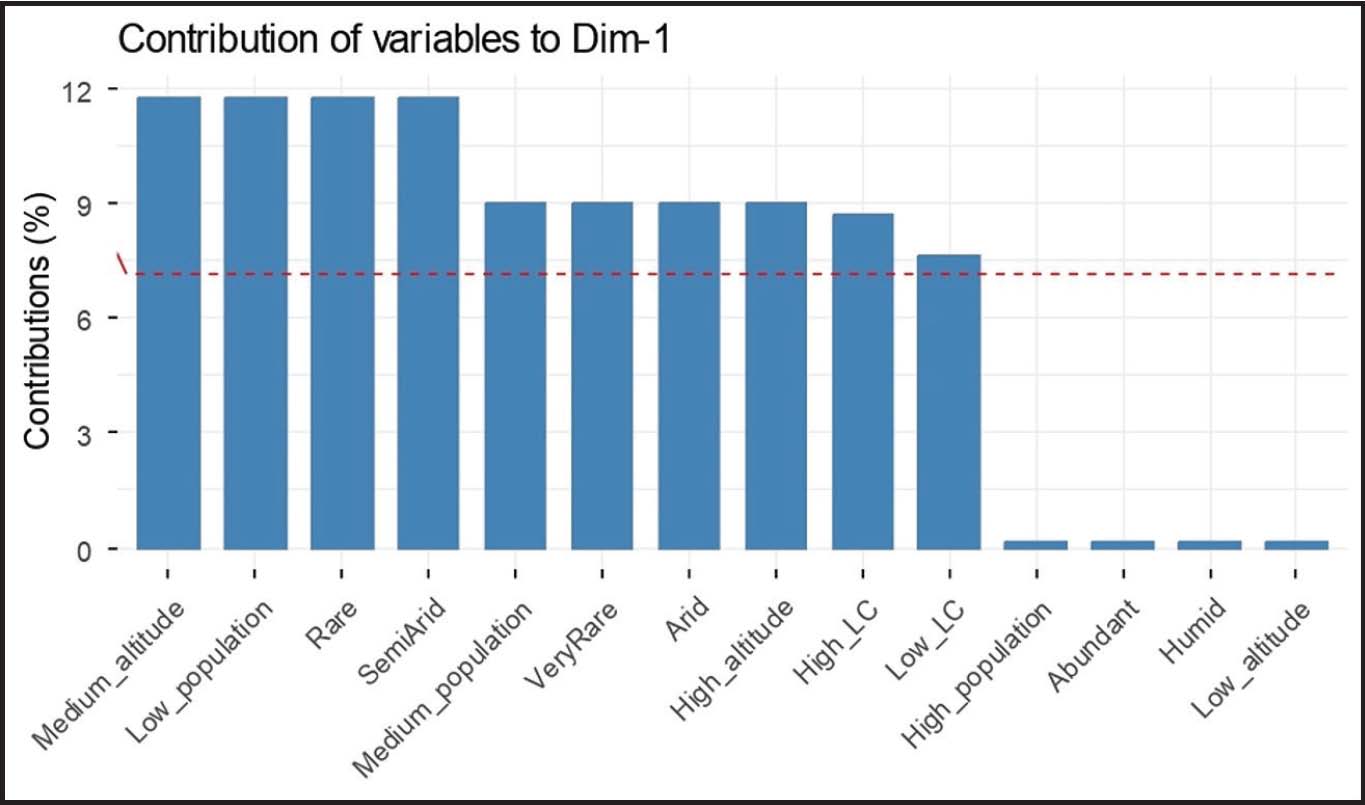
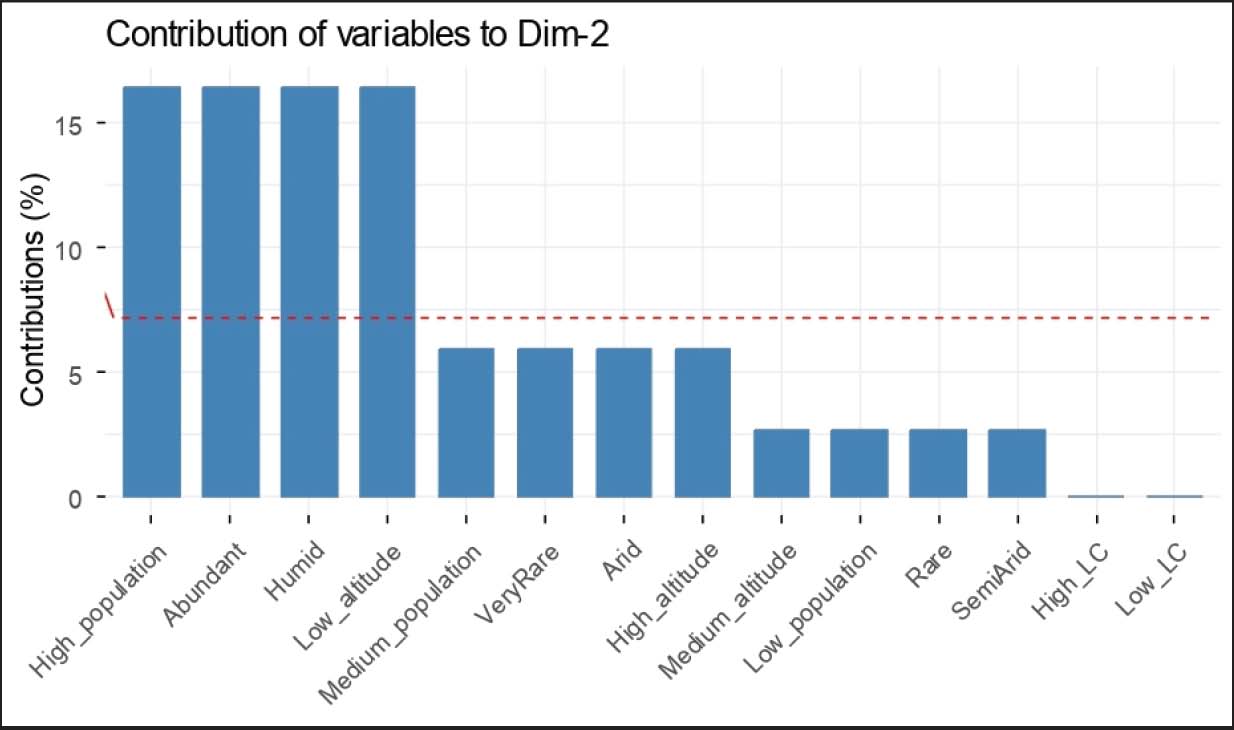
A Kruskal-Wallis test (non-normal distribution) was used to compare the prevalence of sandflies and CL incidence among the three regions in 2020. The results revealed a highly significant difference in sandfly abundance across the regions (χ²=21.02, p < 0.001) as well as a highly significant difference in CL incidence (χ²=27.05, p < 0.001). However, examination of the relationship between CL incidence and sandfly abundance during the study period was not significantly correlated (Spearman’s correlation coefficient, r ≤ 0.05; p > 0.05). Univariate Poisson regression analysis revealed a significant negative association between sandfly abundance and CL incidence (IRR=0.946, 95% CI: 0.943–0.949, p < 0.001). This indicates that higher sandfly abundance does not correspond to higher CL incidence in this dataset, which does not support the expected positive epidemiological association. Impact of the geographic parameters of the three study regions on the CL incidenceUnivariate analyses were conducted to evaluate the potential risk factors for high CL incidence. The population size (IRR=0.99974, 95% CI: 0.99973–0.99975) and altitude (IRR=1.0007, 95% CI: 1.0006–1.0007) showed minimal effects on CL risk. In contrast, ecological factors were strongly associated with the occurrence of CL. Regions with “Rare” vegetation had higher odds of elevated CL cases (odds ratio [OR]=15.40, 95% CI: 0.95–2405.92), whereas “Very Rare” vegetation showed lower odds (OR=0.127, 95% CI: 0.0008–2.21). Climatic zones were also influential: semi-arid areas exhibited markedly higher odds of high CL incidence (OR=121.0, 95% CI: 4.58–40,392.65) and humid areas showed increased odds compared to arid zones (OR=7.86, 95% CI: 0.45–1219.53). These results showed that vegetation and climatic zone are key ecological determinants of CL, whereas population and altitude have a limited impact. The MCA revealed a clear structuring of CL incidence according to ecological and geographic parameters. The first two dimensions explained 96.9% of the total inertia (Dim1=52.5%, Dim2=44.4%) (Fig. 4), indicating a strong representation of the data in two dimensions. Dimension 1 (Figs. 4 and 5) reflects a geographic parameter that separates humid, low-altitude environments with abundant vegetation, high population density, and low CL incidence from semi-arid and arid environments with medium to high altitude, sparse vegetation, lower population density, and higher CL incidence. Dimension 2 (Figs. 4 and 6) emphasizes environmental constraints, with arid conditions, rare to very rare vegetation, and higher altitude associated with increased CL incidence, whereas humid and vegetated environments correspond to lower incidence. Overall, the MCA indicates that climate, vegetation, altitude, and geographic conditions are key determinants of CL distribution across the studied regions.
Fig. 4. MCA biplot of geographic parameters and CL incidence in the three study regions.
Fig. 5. Contribution of variables to Dim-1 in MCA.
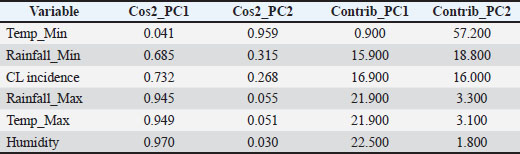
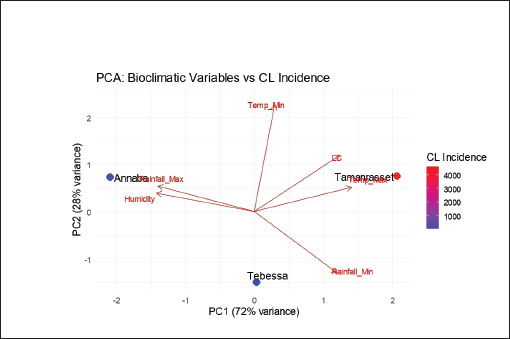
Fig. 6. Contribution of variables to Dim-2 in MCA. Influence of bioclimatic variables on CL incidencePrincipal Component Analysis (PCA) of bioclimatic variables and CL incidence across three regions showed that the first two components explained 72% and 28% of the total variance, respectively (Fig. 7). The first principal component (PC1) was mainly driven by humidity, maximum temperature, maximum rainfall, and CL incidence, all with high quality of representation (cos² > 0.94) and strong contributions (>21%) (Table 5) indicating that these variables are key drivers of the main climatic gradient. Regions characterized by higher temperatures and lower humidity, such as Tamanrasset, formed a distinct climatic cluster in the PCA. However, the highest CL incidence was recorded in Tebessa rather than in Tamanrasset, indicating that these climatic conditions alone do not fully explain disease occurrence. Instead, CL incidence appears to be influenced by a combination of environmental and ecological factors associated with semi-arid regions. The second component (PC2) was mainly driven by the minimum temperature (cos²=0.96; contribution=57%) (Table 5), which largely captured the climatic variation independent of the CL incidence. Overall, these results indicate that the incidence of CL is primarily associated with the combined gradient of humidity and maximum temperature, while the minimum temperature contributes mainly to secondary climatic variation. Table 5. Cos² and contribution of variables to principal components (PC1 and PC2).
Fig. 7. Projection of bioclimatic parameters from the three study regions onto the plane defined by the first two principal components (PC1 and PC2) of the PCA based on the incidence matrix of CL and bioclimatic variables. DiscussionThe survey conducted in the regions of Annaba, Tebessa, and Tamanrasset showed that the total number of CL cases recorded between 2019 and 2023 was 96, 4,596, and 40, respectively. These results indicate that CL is endemic in the semi-arid region of Tebessa, and remains sporadic in the humid region of Annaba and the arid region of Tamanrasset. According to the CL is more widely distributed in the Americas, the Mediterranean Basin, and western Asia, extending from the Middle East to Central Asia. The ten countries with the highest estimated case counts, Afghanistan, Algeria, Iran, Syria, India, Colombia, Brazil, Panama, and Peru, account for approximately 70%–75% of the global estimated incidence of CL (Alvar et al., 2012). The present survey shows that the mean number of CL cases in the Tebessa region during 2010–2018 and 2019–2023 remained very similar despite the different time periods considered. This pattern reflects a persistent endemic level, with a recent increase likely related to the region’s geoclimatic characteristics and the continued presence and proliferation of the parasite and its vector. The present study revealed that the highest incidence occurred in the Tebessa region, which is located at an intermediate latitude (35°24′19″) between the other two study sites. The Biskra region in Algeria, where CL (locally known as “clou de Biskra”) has been endemic for decades, lies at a latitude of 34°51′01.37″ (Sergent et al., 1929). CL is endemic in regions with similar latitudes in other Maghreb countries: 33°44′27″ in Morocco (Talbi et al., 2020) and 35°02′17.63″ in Tunisia (Talmoudi et al., 2017). In the Middle East, endemic areas are located at 35°33′5.88″ in Syria (Hayani et al., 2015) and 34°31′01″ in Iran (Parvizi et al., 2012). Similarly, in Asia, CL occurs mainly around 34°31′01″ in Afghanistan (Adegboye and Adegboye, 2017) and 34°08′36.56″ in India (Rathera et al., 2020). These findings showed that endemic regions are generally aligned along a narrow latitudinal band between 33°44′27″ and 35°33′06″. No clear correlation was observed between longitude, altitude, and CL prevalence. However, the semi-arid landscape of Tebessa, with sparse vegetation, appears to favor CL transmission compared with the humid region of Annaba and the arid desert environment of Tamanrasset. Ghardaïa, another Algerian region where CL is highly prevalent, presents similar geographical features (Saadane et al., 2023). In Syria, CL, also known as the “Aleppo boil,” occurs in the semi-arid zones of Aleppo (Hayani et al., 2015). Comparable patterns have been reported in Sidi Bouzid, Tunisia (Talmoudi et al., 2017), Aichoun, Morocco (Talbi et al., 2020), Natanz, Iran (Parvizi et al., 2012), and Kabul, Afghanistan (Adegboye et al., 2019). In contrast, in the New World, CL is mainly found in humid forested regions of South America, where insect density, including sandflies, is extremely high. These conditions represent key risk factors, provided that Leishmania has been historically established in these regions. This is the case in Brazil (Alessi et al., 2009), Venezuela (Chaves and Añez, 2004), and Colombia (Morales et al., 2024). Similarly, the Annaba region, characterized by a humid climate, abundant vegetation, and numerous mosquito species, recorded only sporadic CL cases over the past decade. Mollalo et al. (2014) associated CL incidence with vegetation indices, used as general proxies for climatic changes (including temperature, humidity, and precipitation). They found that most cases occurred in sparsely vegetated or low-density areas. In Europe, CL remains sporadic within Mediterranean countries with dense vegetation and limited sandfly populations. Only 22.6 autochthonous cases are reported annually in southern France (Pasquier et al., 2022). In a long-term assessment, Ready (2010) reported that the risk of Leishmania introduction and spread within the European Union remains low due to the absence of established vectors and reservoir hosts. CL is rarely reported in hyper-arid desert regions, such as Tamanrasset. The absence of Leishmania and sandflies under extreme geoclimatic conditions can explain this. Historical data for Annaba, Tebessa, and Tamanrasset from 2010 to 2018 revealed similar trends to those observed during the present study, with 36, 4,003, and 16 cases, respectively. These findings indicated a stationary clinical CL state in all three regions. A comparable stability has been reported in Tunisia, Morocco, Syria, Iran, India, Brazil, Peru, and Venezuela, where CL incidence has remained steady over the past decade (WHO, 2023). The current study also confirmed that CL is a typically seasonal disease, with an increase in cases during the winter months and a decline during the summer months. This observation is consistent with previous studies (Chaves and Pascual, 2006; Thomson et al., 2008; Toumi et al., 2012). CL has long been associated with climatic factors. Saadane et al. (2023) linked its endemicity to high humidity levels in Algeria. In Tunisia, Toumi et al. (2012) reported that rainfall plays a major role, whereas in Morocco, Talbi et al. (2020) identified temperature as the determining factor. In Iran, Nikonahad et al. (2017) found that soil type and high temperatures are strongly associated with the prevalence of CL. Rodríguez et al. (2013) further supported the existence of a dynamic relationship between climate and disease transmission in Venezuela. However, the global correlation between climatic parameters and CL incidence remains ambiguous. Temperature, humidity, and rainfall data were statistically analyzed but did not show a significant correlation with CL endemicity. This study also found that the number of sandflies decreased between December and February compared with the rest of the year. Talbi et al. (2020) demonstrated a strong positive correlation between temperature and the seasonal distribution of sandflies, whereas relative humidity and wind speed had no significant effect on their abundance. Toumi et al. (2012) provided evidence that CL is strongly influenced by climatic factors that affect sandfly population density. Parvizi et al. (2012) observed that sandfly activity begins in June, ends in November, and peaks in September. Durán-Martínez et al. (2013) noted that sandfly data are scarce in some European regions, making disease surveillance challenging. Furthermore, the lack of correlation between sandfly abundance and CL incidence may primarily depend on the presence and circulation of the parasite rather than solely on vector abundance. This observation should also be interpreted in light of certain limitations, including possible temporal mismatches between vector abundance and reported human cases, and the use of entomological data from a single year. It is important to note that, although this study addresses certain geographic and bioclimatic parameters, other determinants, such as sociodemographic factors and the presence and dynamics of animal reservoirs, may play a crucial role in CL transmission. The potential underreporting of cases, the use of secondary surveillance data, and the high level of data aggregation at the regional scale are some of the relevant limitations of this study. ConclusionThis study demonstrated that CL in Algeria is characterized by long-term epidemiological stability within historically affected regions, despite marked contrasts in climate and environment. Rather than showing clear expansion or decline, the disease persists at relatively constant levels, suggesting the maintenance of well-established transmission systems. The analysis highlights the importance of spatial determinants, particularly latitude and semi-arid ecological conditions, in shaping disease occurrence regional patterns. These factors appear to act along with historical endemicity, reinforcing the CL’s persistence independent of short-term climatic variability. In contrast, variables such as population size and altitude showed limited influence, underscoring the predominance of ecological and geographic constraints. Taken together, these findings showed that CL control cannot rely solely on short-term interventions or climate-based predictions. Control strategies should integrate historical disease patterns, ecological context, and regional specificity. Strengthening long-term surveillance and fostering coordinated action among endemic regions remain essential for limiting transmission and addressing the sustained public health burden of CL. AcknowledgmentsThis study was fully supported by the Laboratory of Ecology of Terrestrial and Aquatic Systems, University of Badji Mokhtar, Annaba 23000, Algeria. We thank the General Direction of Scientific Research and Technological Development (DGRSTD). FundingThis research received no specific grant. Authors’ contributionsMZ and LB contributed to the study conception, investigation, and supervision. AC and AB conducted the epidemiological and statistical analyses. BZ and MZ developed the methodology. MZ, AC, and AB drafted the manuscript. All authors participated in writing, reviewing, and editing the manuscript. Conflict of interestThe authors declare that there is no conflict of interest. Data availabilityAll data supporting the findings of this study are available within the manuscript. ReferencesAdegboye , M.A., Olumoh, J., Saffary, T., Elfaki, F. and Adegboye, O.A. 2019. Effects of time-lagged meteorological variables on attributable risk of leishmaniasis in central region of Afghanistan. Sci. Total Environ. 685, 533–541; doi:10.1016/j. scitotenv.2019.05.401 Adegboye, O. and Adegboye, M. 2017. Spatially correlated time series and ecological niche analysis of cutaneous leishmaniasis in Afghanistan. Int. J. Environ. Res. Public. Health. 14(3), 309; doi:10.3390/ijerph14030309 Alessi, C.A.C., Galati, E.A.B., Alves, J.R. and Corbett, C.E.P. 2009. American cutaneous leishmaniasis in the Pontal of Paranapanema - SP, Brazil: ecological and entomological aspects. Rev. Inst. Med. Trop. São. Paulo. 51, 277–282; doi:10.1590/s0036-46652009000500008 Alvar, J., Vélez, I.D., Bern, C., Herrero, M., Desjeux, P., Cano, J., Jannin, J. and Boer, M.D. 2012. Leishmaniasis worldwide and global estimates of its incidence. PLos One. 7(5), e35671; doi:10.1371/journal.pone.0035671 Chaves, L.F. and Añez, N. 2004. Species co-occurrence and feeding behavior in sand fly transmission of American cutaneous leishmaniasis in western Venezuela. Acta Trop. 92(3), 219–224; doi:10.1016/j.actatropica.2004.08.001 Chaves, L.F. and Pascual, M. 2006. Climate cycles and forecasts of Cutaneous Leishmaniasis, a nonstationary vector-borne disease. PLos Med. 3(8), 295. Dedet, J.P., Addadi, K., Belazzoug, S., Dib, D., Knidler, B. and Touami, M. 1984. Les phlébotomes (Diptera, Psychodidae) d’Algérie. Cahiers ORSTOM. Série Entomologie Médicale Et Parasitologie 22(2), 99–127. Durán-Martínez, M., Ferroglio, E., Acevedo, P., Trisciuoglio, A., Zanet, S., Gortázar, C.,and Ruiz-Fons, F.2013. Leishmania infantum (Trypanosomatida:Trypanosomatidae) Phlebotomine Sand Fly Vectors in Continental Mediterranean Spain. Environ. Entomol. 6, 1157–1165. DOI: 10.1603/EN13018, 2-s2.0-84891100406, 24128871. Garni, R., Tran, A., Guis, H., Baldet, T., Benallal, K., Boubidi, S. and Harrat, Z. 2014. Remote sensing, land cover changes, and vector-borne diseases: use of high spatial resolution satellite imagery to map the risk of occurrence of cutaneous leishmaniasis in Ghardaïa, Algeria. Infect. Genet. Evol. 28, 725–734; doi:10.1016/j.meegid.2014.09.036 Hayani, K., Dandashli, A. and Weisshaar, E. 2015. Cutaneous leishmaniasis in Syria: clinical features, current status and the effects of war. Acta Dermato-venereologica 95(1), 62–66. Maroli, M., Feliciangeli, M.D., Bichaud, L., Charrel, R.N. and Gradoni, L. 2013. Phlebotomine sandflies and the spreading of leishmaniasis and other diseases of public health concern. Med. Vet. Entomol. 27(2), 123–147; doi:10.1111/j.1365-2915.2012.01034.x Mollalo, A., Alimohammadi, A., Shahrisvand, M., Reza Shirzadi, M. and Reza Malek, M. 2014. Spatial and statistical analyses of the relations between vegetation cover and incidence of cutaneous leishmaniasis in an endemic province, northeast of Iran. Asian Pacific J. Tropic. Dis. 4(3), 176–180. Morales, D.M., Daza, F.S., Betancur, O.F., Guevara, D.M. and Liscano, Y. 2024. The impact of climatological factors on the incidence of cutaneous leishmaniasis (CL) in Colombian Municipalities from 2017 to 2019. Pathogens 13(6), 462; doi:10.3390/pathogens13060462 Nikonahad, A., Khorshidi, A., Ghaffari, H.R., Aval, H.E., Miri, M. and Amarloei, A. 2017. A time series analysis of environmental and meteorological factors’ impact on cutaneous leishmaniasis incidence in an endemic area of Dehloran, Iran. Environ. Sci. Pollut. Res. Int. 24(16), 14117–14123. Parvizi, P., Akhoundi, M. and Mirzaei, H. 2012. Distribution, fauna and seasonal variation of sandflies, simultaneous detection of nuclear internal transcribed spacer ribosomal DNA geneof Leishmania major in Rhombomysopimus and Phlebotomus papatasi, in Natanz District in central part of Iran. Iran. Biomed. J. 16(2), 113–120; doi:10.6091/ibj.1038.2012. Pasquier, G., Demar, M., Lami, P., Zribi, A., Marty, P., Buffet, P., Desbois-Nogard, N., Gangneux, J.P., Simon, S., Blaizot, R., Couppié, P., Thiebaut, L., Pratlong, F., Dedet, J.P., Bastien, P., Sterkers, Y., Ravel, C. and Lachaud, L. 2022. Leishmaniasis epidemiology in endemic areas of metropolitan France and its overseas territories from 1998 to 2020. PLos Neglected Trop. Dis. 16(10), e0010745. Rather, S., Wani, M., Shah, F.Y., Bashir, S., Yaseen, A., Giri, F.A., Sharma, R., Zeerak, S., Jabeen, Y., Hassan, I., Dogra, D. and Rishi, R. 2020. Clinical and epidemiological study of cutaneous leishmaniasis in two tertiary care hospitals of Jammu and Kashmir: an emerging disease in North India. Int. J. Infect. Dis. 103, 138–145. Ready, P.D. 2010. Leishmaniasis emergence in Europe. Euro. Surveill. 11(15), 10. Rodríguez, E.M., Díaz, F. and Pérez, M.V. 2013. Spatio-temporal clustering of American Cutaneous Leishmaniasis in a rural municipality of Venezuela. Epidemics 5(1), 11–19. Saadene, Y., Salhi, A., Mliki, F. and Bouslama, Z. 2023. Climate change and cutaneous leishmaniasis in the province of Ghardaïa in Algeria: a model-based approach to predict disease outbreaks. Ann. Saudi. Med. 43(5), 263–276. Sergent, E.T., Sergent., Parrot, L., Donatien, A. and Beguet, M. 1921. Transmission du clou de Biskra par le phlébotome (Phlebotomus papatasi Scop.). CR. Acad. Sci. 173, 1030. Steverding, D. 2017. The history of leishmaniasis. Parasit. Vectors. 10(1), 82; doi:10.1186/s13071-017-2028-5 Talbi, F.Z., El Ouali Lalami, A., Fadil, M., Najy, M., Ech-Chafay, H., Lachhab, M., Lotfi, S., Nouayti, N., Lahouiti, K., Faraj, C. and Janati Idrissi, A. 2020. Entomological Investigations, Seasonal Fluctuations and Impact of Bioclimate Fac¬tors of Phlebotomines Sand Flies (Diptera: psychodidae) of an Emerging Focus of Cuta¬neous Leishmaniasis in Aichoun, Central Mo¬rocco. J. Parasit. Res. 1(1), 6495108; doi:10.1155/2020/6495108 Talmoudi, K., Bellali, H., Ben-Alaya, N., Saez, M., Malouche, D. and Chahed, M.K. 2017. Modeling zoonotic cutaneous leishmaniasis incidence in central Tunisia from 2009-2015: forecasting models using climate variables as predictors. Trop. Dis. 11(8), e0005844; doi:10.1371/journal.pntd.0001633 Thomson, M.C., Garcia-Herrera, R., Beniston, M., Kelly-Hope, L. and Thomson, M.C. 2008. Seasonal forecasts, climatic change and human health. Springer Science + Business Media B.V. Toumi, A., Chlif, S., Bettaieb, J., Alaya, N.B., Boukthir, A., Ahmadi, Z.E. and Salah, A.B. 2012. Temporal dynamics and impact of climate factors on the incidence of Zoonotic Cutaneous Leish¬maniasis in central Tunisia. PLos Neglected Trop. Dis. 6(5), 1633; doi:10.1371/journal.pntd.0001633 WHO. 2023. Control of Neglected Tropical Diseases (NTD). Operational manual on leishmaniasis vector control, surveillance, monitoring and evaluation, p.119. WHO. 2010. Control of the leishmaniases: report of a meeting of the WHO Expert Committee on the Control of Leishmaniases, Geneva, Switzerland: WHO, pp: 22–26. | ||

| How to Cite this Article |
| Pubmed Style Bouzabata L, Zeghdoudi M, Chettibi A, Bouzabata A, Bouslama Z. Epidemiological study of cutaneous leishmaniasis in Algeria. Open Vet. J.. 2026; 16(5): 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 Web Style Bouzabata L, Zeghdoudi M, Chettibi A, Bouzabata A, Bouslama Z. Epidemiological study of cutaneous leishmaniasis in Algeria. https://www.openveterinaryjournal.com/?mno=299836 [Access: June 26, 2026]. doi:10.5455/OVJ.2026.v16.i5.23 AMA (American Medical Association) Style Bouzabata L, Zeghdoudi M, Chettibi A, Bouzabata A, Bouslama Z. Epidemiological study of cutaneous leishmaniasis in Algeria. Open Vet. J.. 2026; 16(5): 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 Vancouver/ICMJE Style Bouzabata L, Zeghdoudi M, Chettibi A, Bouzabata A, Bouslama Z. Epidemiological study of cutaneous leishmaniasis in Algeria. Open Vet. J.. (2026), [cited June 26, 2026]; 16(5): 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 Harvard Style Bouzabata, L., Zeghdoudi, . M., Chettibi, . A., Bouzabata, . A. & Bouslama, . Z. (2026) Epidemiological study of cutaneous leishmaniasis in Algeria. Open Vet. J., 16 (5), 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 Turabian Style Bouzabata, Leila, Mourad Zeghdoudi, Ahlem Chettibi, Amel Bouzabata, and Zihed Bouslama. 2026. Epidemiological study of cutaneous leishmaniasis in Algeria. Open Veterinary Journal, 16 (5), 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 Chicago Style Bouzabata, Leila, Mourad Zeghdoudi, Ahlem Chettibi, Amel Bouzabata, and Zihed Bouslama. "Epidemiological study of cutaneous leishmaniasis in Algeria." Open Veterinary Journal 16 (2026), 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 MLA (The Modern Language Association) Style Bouzabata, Leila, Mourad Zeghdoudi, Ahlem Chettibi, Amel Bouzabata, and Zihed Bouslama. "Epidemiological study of cutaneous leishmaniasis in Algeria." Open Veterinary Journal 16.5 (2026), 2812-2822. Print. doi:10.5455/OVJ.2026.v16.i5.23 APA (American Psychological Association) Style Bouzabata, L., Zeghdoudi, . M., Chettibi, . A., Bouzabata, . A. & Bouslama, . Z. (2026) Epidemiological study of cutaneous leishmaniasis in Algeria. Open Veterinary Journal, 16 (5), 2812-2822. doi:10.5455/OVJ.2026.v16.i5.23 |

