




| Case Report | ||
Open Vet. J.. 2026; 16(2): 1389-1393
Open Veterinary Journal, (2026), Vol. 16(2): 1389-1393 Case Report Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case reportAgus Wijaya1 and Muchammad Yunus2*1Department of Clinic, Reproduction and Pathology, Veterinary Internal Medicine Division, Faculty of Veterinary Medicine, IPB University, Bogor, Indonesia 2Division of Veterinary Parasitology, Department of Veterinary Science, Faculty of Veterinary Medicine, Universitas Airlangga, Surabaya, Indonesia *Corresponding Author: Muchammad Yunus. Department of Veterinary Science, Faculty of Veterinary Medicine, Universitas Airlangga, Surabaya, Indonesia. Email: muchammad-y [at] fkh.unair.ac.id Submitted: 21/09/2025 Revised: 25/12/2025 Accepted: 09/01/2026 Published: 28/02/2026 © 2026 Open Veterinary Journal
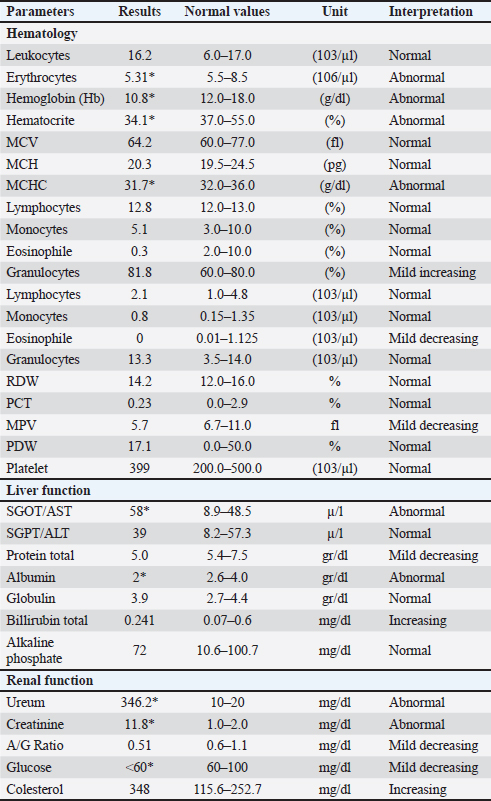
AbstractBackground: Chronic kidney disease (CKD) is a common and progressive disorder in dogs characterized by irreversible loss of renal function over time. It is frequently observed in geriatric dogs and may present with nonspecific clinical signs that require careful diagnostic evaluation for confirmation. Case Description: An 11-year-old male mixed-breed dog weighing 17.9 kg presented with a history of lethargy and anorexia for three consecutive days. On physical examination, the dog had a body temperature of 37.9°C, heart rate of 60 beats per minute (bradycardia), and respiratory rate of 24 breaths per minute (within normal range). Physical examination and clinical laboratory testing, including hematology and serum biochemistry, were performed to evaluate renal function. The results of these investigations, along with the clinical signs, were consistent with CKD. Conclusion: This case highlights the clinical presentation and diagnostic process of CKD in a geriatric mixed-breed dog. Early recognition and appropriate diagnostic evaluation are essential for the accurate diagnosis and management of CKD in dogs. Keywords: CKD, Physical examination, Clinical laboratory tests. IntroductionChronic kidney disease (CKD) is a progressive and irreversible kidney disorder characterized by the gradual loss of functional nephrons and declining renal function over time. It is considered one of the most common causes of morbidity and mortality in geriatric dogs. Epidemiological studies have reported that the prevalence of CKD in dogs can reach up to 25% of patients referred to veterinary institutions (Barlett et al., 2010; Pelander et al., 2015). This high prevalence highlights the importance of early detection, accurate staging, and comprehensive management strategies to improve patient outcomes. From a pathophysiological perspective, CKD is marked by a reduction in the glomerular filtration rate (GFR), impaired renal concentrating ability, and progressive fibrosis of renal tissue. The disease is dynamic, with compensatory adaptations occurring in the remaining functional nephrons, which eventually become overwhelmed, leading to progressive renal insufficiency. This results in various systemic consequences, including azotemia, electrolyte imbalances, metabolic acidosis, hypertension, and renal secondary hyperparathyroidism (Polzin, 2007). The clinical manifestations of CKD are often nonspecific in the early stages, making diagnosis challenging. Common signs include polyuria, polydipsia, anorexia, weight loss, vomiting, lethargy, and oral ulceration, reflecting the accumulation of metabolic toxins and disturbances in water and electrolyte balance (Cathy, 2008). Laboratory abnormalities, such as elevated BUN and serum creatinine, hyperphosphatemia, anemia, and isosthenuria, are typically used to support the diagnosis and assess disease severity. The International Renal Interest Society (IRIS) staging system is widely used to classify CKD severity and guide treatment decisions. The management of CKD in dogs is directed toward several key objectives, such as amelioration of clinical signs of uremia and improvement of quality of life, minimization of metabolic and electrolyte disturbances, including derangements of water, phosphorus, potassium, and acid–base balance, support of adequate nutrition through dietary modification to provide sufficient calories, essential amino acids, and micronutrients, Alfarisa and Soedarmanto, (2017) while restricting phosphorus and protein to slow disease progression, slowing the progression of renal failure by controlling hypertension, proteinuria, and secondary metabolic complications (Polzin, 2007; Cathy, 2008). Because CKD is inherently progressive and dynamic, optimal management requires individualized therapeutic plans based on the clinical stage of the disease, laboratory findings, and patient-specific needs. Serial monitoring is a critical aspect of management, enabling clinicians to modify therapy as the disease progresses or complications raise (Roudebush et al., 2010). CKD in dogs represents a significant clinical challenge because of its high prevalence, progressive nature, and multisystemic effects. Early recognition, accurate staging, and continuous reassessment form the cornerstone of effective management strategies aimed at maintaining patient well-being and prolonging survival. Case DetailsA dog came to the Teaching Animal Hospital, Faculty of Veterinary Medicine, IPB University with some complaints, such as a lack of appetite for 3 days and a weak body. The dog’s name is Koko, a mix breed, 11 years old, male, and his body weight was 17.9 kg. His body temperature was 37.9°C, heart rate was 60 x/minute, and respiration rate was 24 x/minute. A physical was examined to identify clinical findings. Physical examination was performed based on a previous study (Polzin, 2011). Some clinical findings were found, such as a uric smell from his mouth, lethargy, dehydration, anorexia, and vomiting. Clinical findings such as lethargy, no appetite, and vomiting are caused by some factors, for example, the obstruction of the digestive tract, pharyngitis, gastritis, and chronic kidney failure. Some clinical laboratory tests, such as hematological profile and blood biochemical tests, were used. Some tests are needed to identify the causal agent and diagnose the diseases. A male mixed-breed dog named Koko, aged 11 years and weighing 17.9 kg, was presented to the Teaching Animal Hospital, Faculty of Veterinary Medicine, IPB University with a history of inappetence for 3 days and progressive weakness. According to the owner, the dog showed a noticeable decline in activity and had not adequately consumed food during that period. On physical examination, the dog appeared lethargic and weak, with a body temperature of 37.9°C, heart rate of 60 beats per minute, and respiratory rate of 24 breaths per minute. The recorded heart rate indicated mild bradycardia, which may be associated with systemic metabolic disturbances or electrolyte imbalances, which are often seen in patients with CKD. The body temperature of the dogs was slightly below the normal range (38.0°C–39.2°C), possibly due to metabolic depression. Further examination revealed several significant clinical findings, including a uremic odor emanating from the mouth, dehydration, anorexia, and vomiting. Uremic breath and dehydration were suggestive of azotemia and loss of fluid balance, common sequelae in dogs with impaired renal function. These clinical signs, particularly lethargy, loss of appetite, and vomiting, can indicate several conditions, such as gastrointestinal obstruction, pharyngitis, gastritis, or CKD (Polzin, 2011). Clinical laboratory evaluations were conducted to confirm the underlying cause and establish a definitive diagnosis. These included a complete hematological profile and blood biochemical analyses to assess parameters related to renal function, such as BUN, creatinine, electrolyte balance (Na+, K+, Cl−), and hematocrit levels. These diagnostic tests were essential for differentiating between possible systemic causes and for confirming CKD as the primary disorder affecting the patient. Ethical approvalThis case report was approved by the Ethics Committee of the School of Veterinary Medicine and Biomedical Science, IPB University, and was conducted in accordance with the ethical guidelines for animal research. The animal owner provided written informed consent for the use of clinical data and documentation in this study. DiscussionHematology profile and blood biochemical test, Combur test, refractometry of urine sample, and blood tension test were performed as supporting diagnosis. The clinical findings of the patient (Koko) resembled those of CKDs, such as anorexia, vomiting, body weight loss, pale mucous membrane, ulcerative mouth mucous membrane, and halitosis. CKD is a progressive and irreversible renal function disorder in which the body fails to maintain the metabolism or balance of body liquid or electrolyte, ultimately causing uremic syndrome. Generally, older dogs or cats undergo chronic kidney disorder, and their clinical symptoms appear if 75 % of the kidney function is lost. Some clinical symptoms, such as polyuria, polydipsia, anorexia, vomiting, body weight loss, pale mucous membrane, ulcerative mouth mucous membrane, halitosis, and acute blindness, will be found (Yanuartono et al., 2017). According to the International Renal Interest Society (2019), the classification of CKDs can be divided into 1–4 stages, with the highest classification showing the highest decrease in renal function. Stage determination is based on the results of clinical laboratory tests, such as complete blood counting, blood biochemistry, and urinalysis. Dogs suffering from CKDs generally show azotemia. Based on Koko’s blood biochemical tests, his uric acid value was approximately 15-fold (346.2 mg/dl) higher than normal (10–20 mg/dl), and his creatinine level was 6-fold (11.8 mg/dl) higher than normal (1.0–2.0 mg/dl) (Table 1). An increase in uric and creatinine values higher than normal is called azotemia (Audrey et al., 2007). Urinalysis is an essential diagnostic component in the evaluation of CKD in dogs, as it provides valuable information regarding renal structural and functional integrity. The common urinalysis abnormalities observed in canine CKD include proteinuria, hematuria, and leukocyturia, which reflect glomerular damage and chronic inflammatory processes within the kidneys (International Renal Interest Society (IRIS), 2023). Table 1. Hematological profile and biochemical blood tests of the dog.
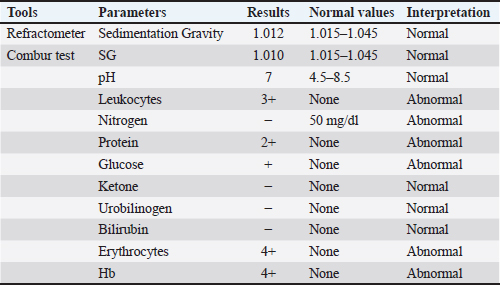
Proteinuria is one of the most clinically significant urinalysis findings in dogs with CKD and is primarily associated with glomerular injury. Disruption of the glomerular filtration barrier increases the permeability of plasma proteins, particularly albumin, allowing their passage into the urine. Persistent proteinuria promotes tubulointerstitial inflammation and fibrosis and contributes to CKD progression. The degree of proteinuria is widely recognized as an important prognostic indicator and a therapeutic target in the management of canine CKD. Hematuria, defined as the presence of erythrocytes in the urine sediment, is commonly detected in dogs with CKD and is typically microscopic. It may be caused by glomerular damage, tubulointerstitial inflammation, or renal vascular injury. (Nicolle et al., 2007). Hematuria may also be associated with concurrent conditions such as urinary tract infection or urolithiasis in some cases. Hematuria indicates ongoing tissue injury within the kidneys or urinary tract associated with chronic renal disease. Leukocyturia reflects the presence of leukocytes in the urine and indicates inflammation or infection within the kidneys or urinary tract. Leukocyturia in dogs with CKD may result from chronic interstitial nephritis or secondary urinary tract infections due to impaired urinary defense mechanisms. This finding suggests the involvement of the TICC in the pathophysiology of CKD. The increase in these values was caused by the decrease GFR or kidney nephron excretion and absorption function failure. The decreased GFR in canine CKD leads to phosphorus retention and decreased serum calcium levels, which in turn stimulates increased parathyroid hormone secretion and leads to secondary renal hyperparathyroidism. This disturbance in calcium–phosphorus metabolism plays a crucial role in the pathophysiology and progression of CKD and is an important target in the clinical management of CCKD. The increase in serum uric acid can result in some clinical symptoms, such as anorexia, nausea, and vomiting. Severe CKD results in increased protein excretion and hypertension (Leyenda and Cathy, 2012). Koko suffered from renal azotemia. Anemia is a clinical symptom of CKD. Three parameters of anemia evaluation are hemoglobin, erythrocytes, and hematocrit values. The complete blood count of Koko’s blood sample showed that Hb (10.8 g/dl) was lower than normal (12.0–18.0 g/dl), erythrocytes 5.31 (106/µl) was lower than normal condition 5.5–8.5 (106/µl), and hematocrit (34.1 %) was lower than normal (37.0%–55.0%) (Table 1). The type of CKD anemia is usually non-regenerative anemia due to kidney failure (Grimes and Fry, 2015). Examination of sedimentation gravity by refractometer and Combur tests showed normal condition (Table 2). Koko’s blood systole average was 167 mmHg, and it was done four times with an interval time of approximately 30 minutes (Table 3). According to IRIS 2019, the normal dog blood pressure is around <150-mm Hg. Table 2. Urinalysis of the urine sample of the dog (Koko) (refractometer and Combur tests).
Table 3. Koko’s blood pressure examination results.
ConclusionSome clinical signs of CKD are observed in dogs that come to the animal teaching hospitals of the Faculty of Veterinary Medicine of IPB University. Physical and laboratory examinations were then performed on the dog. The examination results confirmed the clinical presentation and diagnostic process of CKD in a geriatric mixed-breed dog. Early recognition and appropriate diagnostic evaluation are essential for the accurate diagnosis and management of CKD in dogs. AcknowledgmentThe authors are grateful to the Teaching Animal Hospital, Faculty of Veterinary Medicine, IPB University, particularly the Veterinary Internal Medicine Division, Department of Clinic, Reproduction and Pathology, for providing facilities for the examination. FundingThis research did not receive any specific grant from public, commercial, or not-for-profit funding agencies. The case described in this report was observed as part of routine clinical activity at the Veterinary Teaching Hospital, IPB University, without external financial support. Authors’ contributionsAW was responsible for clinical examination, diagnosis, and case data collection. MY contributed to data analysis, manuscript writing, and preparation of the final report. Both authors have read and approved the final version of the manuscript for publication. Conflict of interestThe authors declare no conflicts of interest related to the research, analysis, or publication of this case report. All data and findings are presented objectively without any external influence. Data availabilityAll data supporting this case report’s findings are included within the main text. Additional clinical data or supporting materials are available from the corresponding author upon reasonable request, while maintaining confidentiality of the patient and owner identity in accordance with ethical standards. ReferencesAlfarisa, Y. and Soedarmanto, I. 2017. Chronic kidney disease in dogs and cats: treatment and diet management. JSV 35(1), 16–34. Audrey P.N., Vale´rie, C., Allerheiligen, T., Jean-Louis, P., Gouni, V., Tessier-Vetzel, D., Sampedrano, C. C. and Herve´, P.L. 2007. Azotemia and glomerular filtration rate in dogs with chronic valvular disease. J. Vet. Intern. Med. 21, 943–949. Bartlett, P.C., Van Buren, J.W., Neterer, M. and Zhou, C. 2010. Disease surveillance and referral bias in the veterinary medical database. Prev. Vet. Med. 94(3-4), 264–271. Cathy, L. 2008. Managing fluid and electrolyte disorders in renal failure. Vet. Clin. Small Anim. 38, 677–697. Grimes, C.N. and Fry, M.M. 2015. Nonregenerative anemia: mechanisms of decreased or ineffective erythropoiesis. Vet. Pathol. 52(2), 298–311. International Renal Interest Society (IRIS), 2019. Staging of chronic kidney diseases. Available via http://www.iriskidney.com/guidelines/staging.html International Renal Interest Society (IRIS) (2023). IRIS guidelines for the diagnosis and management of chronic kidney disease in dogs. Paris: International Renal Interest Society. Leyenda, H. and Cathy, L. 2012. Proteinuria in dogs and cats. Can. Vet. J. 53(6), 631–638. Nicolle, A.P., Chetboul, V., Allerheiligen, T., Pouchelon, J.L., Gouni, V., Tessier-Vetzel, D., Sampedrano, C.C. and Lefebvre, H.P. 2007. Azotemia and glomerular filtration rate in dogs with chronic valvular disease. J. Vet. Intern. Med. 21(5), 943–949. Pelander, L., Ljungvall, I., Egenvall, A., Syme, H., Elliott, J. and Häggström, J. 2015. Incidence of and mortality from kidney disease in over 600,000 insured Swedish dogs. Vet. Rec. 176(25), 656. Polzin, D.J. 2007. 11 guidelines for conservatively treating chronic kidney disease. Vet. Med. 102(12), 788–799. Polzin. 2011. Chronic kidney disease in small animals. Vet. Clin. Small Anim. 41, 15–30. Roudebush, P., Polzin, D.J., Adams, L.G., Towell, T.L. and Forrester, S.D. 2010. An evidence-based review of therapies for canine chronic kidney disease. JSAP. 51. 51, 244–252. Yanuartono, Y., Nururrozi, A. and Indarjulianto, S. 2017. Penyakit ginjal kronis pada anjing dan kucing: manajemen terapi dan diet. Jurnal Sain Veteriner 35(1), 16–34. | ||

| How to Cite this Article |
| Pubmed Style Wijaya A, Yunus M. Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Vet. J.. 2026; 16(2): 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 Web Style Wijaya A, Yunus M. Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. https://www.openveterinaryjournal.com/?mno=291818 [Access: February 27, 2026]. doi:10.5455/OVJ.2026.v16.i2.55 AMA (American Medical Association) Style Wijaya A, Yunus M. Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Vet. J.. 2026; 16(2): 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 Vancouver/ICMJE Style Wijaya A, Yunus M. Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Vet. J.. (2026), [cited February 27, 2026]; 16(2): 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 Harvard Style Wijaya, A. & Yunus, . M. (2026) Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Vet. J., 16 (2), 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 Turabian Style Wijaya, Agus, and Muchammad Yunus. 2026. Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Veterinary Journal, 16 (2), 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 Chicago Style Wijaya, Agus, and Muchammad Yunus. "Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report." Open Veterinary Journal 16 (2026), 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 MLA (The Modern Language Association) Style Wijaya, Agus, and Muchammad Yunus. "Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report." Open Veterinary Journal 16.2 (2026), 1389-1393. Print. doi:10.5455/OVJ.2026.v16.i2.55 APA (American Psychological Association) Style Wijaya, A. & Yunus, . M. (2026) Chronic kidney disease in a dog with hematologic and cardiovascular alterations: A case report. Open Veterinary Journal, 16 (2), 1389-1393. doi:10.5455/OVJ.2026.v16.i2.55 |

