




| Case Report | ||
Open Vet. J.. 2026; 16(1): 724-730 Open Veterinary Journal, (2026), Vol. 16(1): 724-730 Case Report Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal ruptureChiara Ferrari, Veronica Cola*, Ilaria Magagnoli, Gaia Costantini, Luca Ciammaichella, Monika Joechler, Gualtiero Gandini and Luciano PisoniDepartment of Veterinary Medical Sciences, University of Bologna, Bologna, Italy *Corresponding Author: Veronica Cola. Department of Veterinary Medical Sciences, University of Bologna, Bologna, Italy. Email: veronica.cola2 [at] unibo.it Submitted: 14/07/2025 Received: 15/11/2025 Accepted: 03/12/2025 Published: 31/01/2026 © 2025 Open Veterinary Journal
AbstractBackground: Vertebral fractures are relatively common in cats, affecting the thoracic or lumbar spine more frequently than the cervical region. Patient history and clinical signs at presentation often guide the initial diagnostic suspicion; however, advanced imaging techniques are usually essential for establishing a definitive diagnosis. The management of these cases is often complex, and not all patients require surgical intervention. When surgery is indicated, the primary goal is to decompress the spinal cord and prevent further secondary injury. Case Description: A 3-year-old female domestic shorthair cat was referred for suspected bite trauma to the neck region. The cat presented with subcutaneous emphysema of the neck and cranial thorax, and pain on manipulation, associated with non-ambulatory tetraparesis, consistent with C1–C5 neurolocalization. Thoracic radiographs confirmed subcutaneous emphysema, pneumomediastinum, and mild pneumothorax, without signs of cervical injuries. Computed tomography (CT) confirmed a vertebral fracture, involving the dorsal lamina of C4, along with tracheal rupture. Surgical treatment via a dorsal approach was performed, and the fractured vertebral fragment was removed to decompress the spinal cord, while the tracheal rupture was managed conservatively. Postoperatively, the cat showed progressive clinical improvement, and 3 months after the trauma, normal ambulation was completely resumed. Conclusion: To the best of the author’s knowledge, this is the first case report describing a C4 vertebral fracture associated with tracheal rupture in a cat, managed successfully through surgical decompression without the need for vertebral stabilization. Diagnosis can be challenging without advanced diagnostic imaging; thus, in this case, the radiographic study failed to detect the vertebral fracture, which was shown only on CT imaging. Establishing a prioritization protocol in patients with multiple concurrent injuries is both challenging and critical, and should be guided by clinical status and imaging findings. Surgical intervention should always be considered for unstable or compressive cervical fractures to avoid secondary neurological deterioration, potentially leading to a rapid and favorable outcome. Keywords: Cervical fracture, Neurosurgery, Spinal cord injury, Tracheal rupture. IntroductionTraumatic spinal cord injury is a significant and relatively common cause of neurological dysfunction in cats, and it is frequently associated with motor vehicle accidents, falls, or bite wounds (Hawthorne et al., 1999; Mella et al., 2020). Thoracolumbar vertebral injuries are more commonly reported, whereas cervical fractures are relatively rare but clinically important events (Hawthorne et al., 1999; Mella et al., 2020). These lesions can result in spinal cord compression and neurological deficits, with the prognosis largely depending on the promptness and adequacy of therapeutic intervention (Hawthorne et al., 1999; Jeffery, 2010). Management of these patients is often challenging and does not always require surgical treatment (Hawthorne et al., 1999; Jeffery, 2010). However, recent studies have increasingly supported the notion that surgical treatment is more effective than a conservative approach for unstable or compressive fractures (Hawthorne et al., 1999; Olby, 2010; Orgonikova et al., 2021). Although uncommon, tracheal injuries in cats have been documented following direct trauma or orotracheal intubation (Hardie et al., 1999; Mitchell et al., 2000). Clinical signs include subcutaneous emphysema, dyspnea, and respiratory stridor (Hardie et al., 1999; Mitchell et al., 2000). Tracheal injuries may be treated conservatively or interventionally, with surgery generally reserved for patients unresponsive to medical management (Hardie et al., 1999; Mitchell et al., 2000). This case report describes a C4 vertebral fracture associated with tracheal rupture in a three-year-old domestic shorthair cat, highlighting the importance of a comprehensive diagnostic approach and timely surgical management to optimize neurological and functional outcomes. Case DetailsA 3-year-old female domestic shorthair cat was referred for a trauma to the neck region, occurring at an unknown time, approximately 24 hours before the cat was rescued. Upon admission, the cat was normothermic, normotensive, with a heart rate of 200 beats per minute, and tachypneic with a respiratory rate of 44 breaths per minute. The breathing pattern was unremarkable, and pulse oximetry showed oxygen saturation of 97%. The cat had diffuse swelling of the cervical and cranial thoracic region, with a crackling sound on palpation, consistent with subcutaneous emphysema, and pain on manipulation of the neck. No external signs of trauma were evident except for two small contusions on the ventral cervical region. The cat was also markedly obtunded and lay in lateral recumbency. Abdominal focused assessment with sonography in trauma was negative for effusion, whereas thoracic focused assessment with sonography in trauma was unfeasible because of artifacts related to subcutaneous emphysema. Neurological examination revealed non-ambulatory tetraparesis associated with pain, absence of postural reactions on the forelimbs and decreased on the hindlimbs, and preservation of voluntary urination. Spinal reflexes and cranial nerve were normal. Neurological examination was consistent with a C1–C5 neurolocalization. On arrival, venous blood gas analysis revealed mild respiratory acidosis and mild hyperlactatemia (Table 1). The complete blood count revealed moderate thrombocytopenia and neutrophilic leukocytosis (Table 2). Biochemical analysis showed elevated liver and muscular enzyme levels and increased serum amyloid A levels (Table 2). Hypofibrinogenemia (1.36 g/l) with unremarkable coagulation time was evident. All abnormalities were consistent with the traumatic event suspected. Thoracic radiographs confirmed the presence of severe subcutaneous emphysema, associated with moderate pneumomediastinum and mild pneumothorax (Fig. 1). Computed tomography (CT) was scheduled for the following day due to the high suspicion of tracheal injury associated with cervical compressive myelopathy. The cat was hospitalized at the intensive care unit under strict monitoring, minimizing manipulation as much as possible. Fluid therapy was set at 2 ml/kg/h IV of lactated Ringer’s solution, together with analgesic therapy with methadone at 0.1 mg/kg IV every 4 hours, and antibiotic therapy with ampicillin-sulbactam 20 mg/kg IV every 8 hours. The cat was mildly symptomatic for the pneumothorax and was therefore managed conservatively. The following day, the clinical parameters were stable, and a progressive reduction of the subcutaneous emphysema and pneumothorax was noted; therefore, the patient was sedated with 0.2 mg/kg of methadone intravenously (IV) and 2 µg/kg of dexmedetomidine IV, and then placed in a VetMouseTrapTM to avoid intubation and general anesthesia. CT scans confirmed the moderate to severe subcutaneous emphysema, pneumomediastinum, and mild pneumothorax (Fig. 2). A dorsal parietal deformation of the cervical trachea of approximately 1 cm in length was observed, causing a mild reduction in the dorsoventral tracheal diameter. There were no other airway injuries. An incomplete fracture line of the caudal margin of the C4 vertebral arch was observed. The fracture line appeared slightly left-lateralized, with a caudal bone fragment approximately 2 mm long and 5 mm wide. This fragment was dislocated into the vertebral canal, narrowing the dorsoventral diameter, with subsequent compression of the spinal cord (Fig. 3). The CT scan confirmed the suspicion of C4 vertebral fracture and tracheal rupture. Endoscopic evaluation of the upper airways and surgical treatment with a dorsal approach for spinal decompression were scheduled for the following day.
Fig. 1. Thoracic radiography (lateral view) performed upon patient arrival. Note the severe subcutaneous emphysema (white asterisk) in the head and neck region combined with moderate pneumomediastinum and mild pneumothorax.
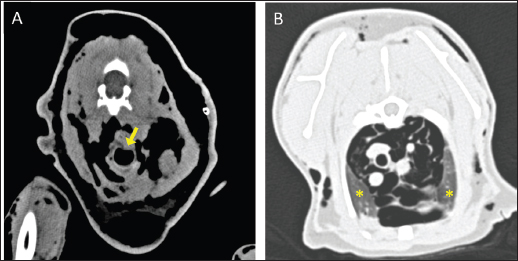
Fig. 2. Transverse CT images acquired with the cat placed in the VetMouse TrapTM. (A) Presence of gas attenuation material in the subcutis around the neck, consistent with subcutaneous emphysema. A dorsal deformation of the cervical trachea with mild reduction of the tracheal diameter is visible in the same scan (A, yellow arrow). (B) The presence of mild pneumo-mediastinum and pneumothorax is further observed, and the collapsed lung lobe is noted (B, yellow asterisk).
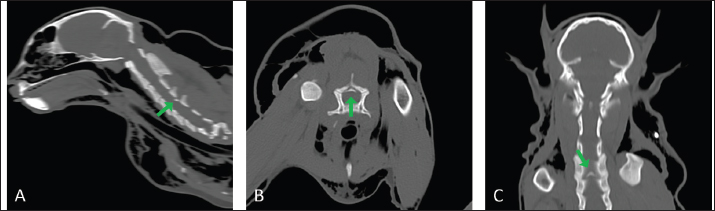
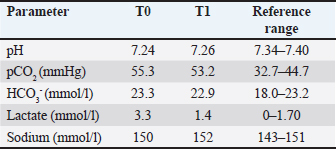
Fig. 3. Longitudinal (A, C) and transverse (B) CT images acquired with the cat placed in the VetMouse TrapTM. Incomplete fracture line of the caudal margin of the fourth cervical vertebral arch (green arrow). The fragment is dislocated into the vertebral canal, narrowing the dorsoventral diameter with subsequent compression of the spinal cord. Table 1. Results of selected clinicopathological variables at blood gas analysis evaluated at different time points in the case described. T0=upon admission; T1=after surgery.
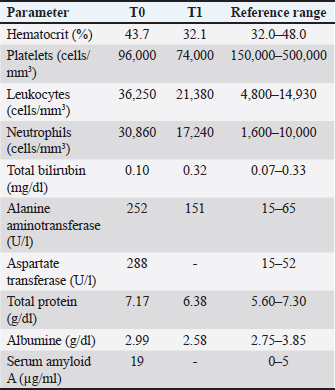
Table 2. Results of selected clinicopathological variables at complete blood count and serum biochemical profile evaluated at different time points in the case described. T0=Day 1, upon admission; T1=Day 3, postoperative.
The cat was premedicated with 5 µg/kg of dexmedetomidine intramuscularly (IM) and 5 mg/kg of ketamine IM, and then induced with propofol IV to effect. The upper respiratory tract was examined endoscopically before intubation, revealing a small amount of fibrin between the third and fourth tracheal rings without an obvious tear, likely representing granulation tissue over a previous tracheal rupture. Subsequently, the cat was intubated, with the endotracheal tube cuff carefully advanced beyond the tracheal lesion under endoscopic guidance. Anesthesia was maintained with isoflurane delivered in a 100% air-oxygen mixture, and the cat was ventilated using intermittent positive pressure ventilation. Broad-spectrum antibiotic prophylaxis with ampicillin-sulbactam at 20 mg/kg IV was administered 30 minutes before skin incision and then every 120 minutes, while fluid therapy was set at 5 ml/kg/h of lactated Ringer’s solution, and analgesic therapy with intravenously constant rate infusions (CRIs) of fentanyl at 5 µg/kg/h plus ketamine at 0.6 mg/kg/h was initiated. The cat was placed in sternal recumbency with the neck gently flexed in a neutral position. The skin was aseptically prepared, and a midline skin incision was made from the atlas to the level of the seventh cervical vertebra to explore the cervical region. The epaxial muscles showed evidence of blunt trauma without signs of direct laceration (Fig. 4A). The nuchal ligament was split longitudinally, and the cervical vertebrae spinous processes were identified. The multifidus muscle was elevated from the spinous processes to expose the dorsal lamina and perform the fourth and fifth cervical vertebrae skeletonization. The bone fracture was then identified at the dorsal lamina’s caudal margin of C4, caudal to the spinous process. The caudal fragment was grasped and elevated with bone forceps (Fig. 4B). The periosteum and ligamentum flavum lateral and caudal to the fragment were then severed and gently removed with a scalpel blade. The spinal cord below the fragment showed no gross alteration or signs of contusion (Fig. 4C). After removing the bone fragment, both fentanyl and ketamine CRIs were gradually tapered, and the cat remained normotensive with a normal heart rate until the end of the surgery. Once the surgical field was irrigated and adequate hemostasis was confirmed, the fascia, subcutaneous tissue, and skin were sutured in a routine fashion.
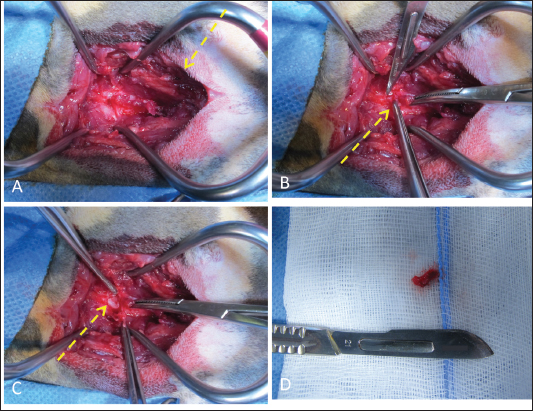
Fig. 4. Surgical approach to vertebral fracture of C4 through a dorsal cervical approach. (A) Once the surgical access was performed, the epaxial muscles showed gross evidence of blunt trauma (yellow dotted arrow). (B) The fourth and fifth cervical vertebrae were skeletonized to evidence the bone fracture. Then, the caudal fragment was grabbed, elevated, and removed, cutting the flavum ligament (note the bone fragment between the forceps, yellow dotted arrow). (C) The uncompressed spinal cord was visualized after the bone fragment was removed (yellow dotted arrow). At the end of the procedure, the cat gradually and quietly awakened. Venous blood gas analysis revealed mild respiratory acidosis and mild hypernatremia, consistent with the results of the anesthetic procedure (Table 1). The cat was monitored in the intensive care unit, and hypotonic fluid therapy was started at 2 ml/kg/h IV, together with analgesic therapy with methadone at 0.1 mg/kg IV every 4 hours, and antiemetic therapy with maropitant at 1 mg/kg IV every 24 hours. Antibiotic therapy with 20 mg/kg IV ampicillin-sulbactam every 8 hours was continued. Almost 12 hours after surgery, the cat positioned itself in sternal recumbency, began eating spontaneously, and maintained spontaneous urination. Over the following days, the cat showed progressive clinical improvement to the point of resumption of ambulation. A complete blood count revealed mild normocytic normochromic anemia, moderate thrombocytopenia, and worsening of neutrophilic leukocytosis (Table 2). Biochemical analysis revealed a decrease in hepatic and muscle damage markers and hypoproteinemia, consistent with trauma sequelae (Table 2). Analgesia was discontinued 72 hours postoperatively, and the cat was discharged with a broad-spectrum antibiotic therapy with amoxicillin and clavulanic acid 20 mg/kg orally every 12 hours for another 5 days, with the recommendation of cage rest for 1 month, followed by appropriate physiotherapy. Given the progressive clinical improvement and the absence of marked postoperative deficits, physiotherapy was declined. After discharge, the cat showed further progressive improvement up to near-normal ambulation at the clinical follow-up 14 days after surgery, despite presenting with residual mild proprioceptive ataxia in the thoracic and pelvic limbs. Breathing patterns were unremarkable, neck manipulation was painless, and the surgical wound had completely healed. Three months after surgery, the cat regained a completely normal gait and returned to its normal lifestyle. DiscussionThis is the first case report describing the clinical presentation and surgical management of a C4 vertebral fracture in a cat. A cascade of pathological processes occurs following traumatic spinal cord injury, including hypoperfusion, rapid changes in intracellular ion concentrations, and the release of reactive oxygen species (Olby, 2010). Additionally, progressive demyelination and worsening of neuronal injury can occur in cases of sustained spinal cord compression (Jeffery, 2010). This mechanism leads to the exacerbation of spinal cord damage and should be interrupted as soon as possible (Olby, 2010). Therefore, the primary goal of surgical intervention is to preserve residual neurological function by decompressing the spinal cord and creating an environment in which the damaged neuronal tissue can heal (Jeffery, 2010). To date, the surgical treatment of vertebral fractures, particularly cervical ones, remains controversial (Hawthorne et al., 1999). This debate stems from the high perioperative mortality rates observed; however, there is increasing evidence suggesting that unstable or compressive fractures would benefit more from surgical treatment than from conservative management (Horlein, 1978; Hawthorne et al., 1999; Olby, 2010; Orgonikova et al., 2021). In this case, surgical intervention effectively relieved the spinal cord compression and prevented secondary neuronal injury, resulting in a rapid and favorable outcome. Surgical treatment of cervical spine fractures generally involves the use of monocortical or bicortical screws and polymethylmethacrylate or locking plates (Hawthorne et al., 1999; Jeffery, 2010; Orgonikova et al., 2021). However, in this case, the fracture consisted of an almost complete fragment of the dorsal lamina, without involvement of the articular processes; therefore, surgical stabilization was deemed unnecessary. Removal of the compressive bone fragment did not result in instability, as the spinal stability was maintained by the vertebral body, articular processes, and intervertebral disc. Therefore, the procedure was comparable to a dorsal laminectomy. The initial radiographic study failed to detect the vertebral fracture in the case reported herein. This is consistent with the known limitations of radiology, which, despite its widespread use, has only moderate sensitivity for the diagnosis of vertebral luxation and fractures and is prone to several artifacts (Kinns et al., 2006; Eminaga et al., 2011). Given these limitations and the strong clinical suspicion of a cervical vertebral fracture or luxation, CT was recommended, confirming a C4 vertebral fracture. Due to its 100% sensitivity and detailed definition of vertebral bony structure, CT is the gold standard for the diagnosis of vertebral fractures (Kinns et al., 2006; Da Costa and Samii, 2010; Orgonikova et al., 2021). In this case, the cat presented with concurrent airway trauma, a finding not uncommon in feline polytraumatized patients with vertebral fractures, where associated injuries are reported in up to 83% of cases (Hawthorne et al., 1999; Bruce et al., 2008; Bali et al., 2009). Although rare in cats, tracheal rupture is a potentially life-threatening condition that may arise from both traumatic and iatrogenic events (Hardie et al., 1999; Bhandal and Alan, 2007). It most commonly affects the extrathoracic portion of the trachea, particularly at the junctions between the tracheal rings and the trachealis muscle, where structural vulnerability is greatest (Bhandal and Alan, 2007). Given the complexity of this presentation, prioritizing clinical interventions was critical. Although standardized guidelines for the management of tracheal injuries in cats are lacking, conservative treatment, including strict cage rest, oxygen supplementation, and sedation, is generally recommended for patients exhibiting mild to moderate clinical signs (Hardie et al., 1999; Mitchell et al., 2000; Bhandal and Alan, 2007). In contrast, surgical repair, which typically involves simple interrupted or continuous sutures with absorbable or nonabsorbable materials, is reserved for cats that fail to respond to medical management or develop progressive respiratory compromise (Hardie et al., 1999; Mitchell et al., 2000; Bhandal and Alan, 2007). The patient also presented with a mild pneumothorax without any thoracic injuries. Pneumothorax may require either conservative management (e.g., drainage and/or monitoring) or interventional treatment (e.g., chest tube insertion and/or management of the underlying cause; e.g., pulmonary injury). In this case, the conservative management elicited for the tracheal laceration was based on the patient’s stable breathing patterns and the apparent healing of the tracheal injury on imaging. The slight pneumothorax was likely secondary to the pneumomediastinum and tracheal injury. Therefore, a conservative approach consisting of strict clinical monitoring without drainage was also adopted for the pneumothorax. This allowed the priority to be given to the cervical fracture. Furthermore, the surgical position required for tracheal exploration may have worsened spinal cord injury, potentially resulting in irreversible consequences. Although the tracheal lesion appeared to be almost healed at the time of endoscopic examination, it is plausible that the tracheal and cervical spine traumas were concomitant. Indeed, the cat exhibited simultaneous and hyperacute neurological and respiratory symptoms, with the onset of subcutaneous emphysema and pneumomediastinum (and subsequent pneumothorax), which spontaneously resolved. The time between the trauma and the endoscopic examination was probably sufficient to allow for initial spontaneous healing of the tracheal lesion. Pain control is another key point that influences the outcome in these cases. The cat appeared to be in significant pain on admission and until spinal cord decompression, showing rapid pain relief after surgery, indicating that the surgical intervention allowed for better pain control. Pain management is crucial for treating any surgical condition, not only for ethical reasons but also for pathophysiological ones. Indeed, pain triggers a series of neuroendocrine responses, culminating in the release of cytokines and catecholamines, which impair immune function and delay wound healing (McGuire et al., 2006). Specifically, the release of cytokines after spinal trauma can lead to hypoperfusion, thereby increasing secondary neuronal damage (Olby, 2010). Thus, effective pain control is essential in the management of these cases to mitigate secondary spinal cord injury (Jeffery, 2010). ConclusionThis case report describes the clinical presentation, diagnostic imaging findings, management, and outcome of a cat with a C4 vertebral fracture and concurrent tracheal rupture. Diagnosis with conventional imaging techniques can be challenging, and in unstable or compressive fractures, surgical intervention should always be considered. Conflict of interestThe authors declare no conflict of interest. FundingThis study received no specific grant. Authors’ contributionsChiara Ferrari contributed to the study’s clinical aspects, collected and managed the documentation, and wrote the manuscript. Veronica Cola contributed to the clinical aspects of the study and wrote and edited the manuscript. Ilaria Magagnoli, Gaia Costantini, and Monika Joechler contributed to the study’s clinical aspects and read and approved the final manuscript. Luca Ciammaichella and Gualtiero Gandini collected and managed the documentation and read and approved the final version of the manuscript. Luciano Pisoni supervised and guided the study, was responsible for the treatment and surgical procedures, and read and approved the final manuscript. Data availabilityAll data supporting this study’s findings are available within the manuscript. ReferencesBali, M.S., Lang, J., Jaggy, A., Spreng, D., Doherr, M.G. and Forterre F. 2009. Comparative study of vertebral fractures and luxations in dogs and cats. Vet Comp Orthop Traumatol. 22, 47–53. Bhandal, J. and Alan, K. 2008. Tracheal rupture in a cat: diagnosis by computed tomography. Can. Vet. J. 49, 595. Bruce, C.W., Barisson, B.A. and Gyselinck, K. 2008. Spinal fracture and luxation in dogs and cats. Vet Comp Orthop Traumatol. 21, 280–284. Da Costa, R.C. and Samii, V.F. 2010. Advanced imaging of the spine in small animals. Vet. Clin. North. Am. Small. Anim. Pract. 40, 765–790. Eminaga, S., Palus, V. and Cherubini, G.B. 2011. Acute spinal cord injury in the cat: causes, treatment and prognosis. J. Feline Med. Surg. 13(11), 850–862. Hardie, E.M., Spodnick, G.J., Gilson, S.D., Benson, J.A. and Hawkins, A.C. 1999. Tracheal rupture in cats: 16 cases (1983–1998). J. Am. Vet. Med. Assoc. 214(4), 508–512. Hawthorne, J.C., Blevins, W.E., Wallace, L.J., Glickman, N. and Waters, D.J. 1999. Cervical vertebral fractures in 56 dogs: a retrospective study. J. Am. Anim. Hosp. Assoc. 35(2), 135–146. Horlein, B.F. 1978. Acute trauma to the central nervous system.In Canine neurology: diagnosis and treatment. Horlein, B.F 3rd, Philadelphia: WB Saunders, pp: 381–405. Jeffery, N.D. 2010. Vertebral fracture and luxation in small animals. Vet. Clin. North Am. Small Anim. Pract. 40, 809–828. Kinns, J., Mai, W., Seiler, G., Zwingenberger, A., Johnson, V., Cáceres, A., Valdés-Martínez, A. and Schwarz, T. 2006. Radiographic sensitivity and negative predictive value for acute canine spinal trauma. Vet. Radiol. Ultrasound. 47(6), 563–570. McGuire, L., Heffner, K., Glaser R Needleman., Malarkey, W., Dickinson, S., Lemeshow, S., Cook, C., Muscarella, P., Melvin, W.S., Ellison, E.C. and Kiecolt-Glaser, J.K. 2006. Pain and wound healing in surgical patients. Ann. Behav. Med. 31(2), 165–172. Mella, S.L., Cardy, T.J., Volk, H.A. and De Decker, S. 2020. Clinical reasoning in feline spinal disease: which combination of clinical information is useful?. J. Feline. Med. Surg. 22(6), 521–530. Mitchell, S.L., McCarthy, R., Rudloff, E. and Pernell, R.T. 2000. Tracheal rupture associated with intubation in cats: 20 cases (1996–1998). J. Am. Vet. Med. Assoc. 216(10), 1592–1595. Olby, N. 2010. The pathogenesis and treatment of acute spinal cord injuries in dogs. Vet. Clin. North. Am. Small. Anim. Pract. 40, 791–807. Orgonikova, I., Brocal, J., Cherubini, G.B. and Palus, V. 2021. Vertebral fractures and luxations in dogs and cats, part 1: evaluation of diagnosis and prognosis. Companion Anim. 26(2), 15–19. | ||

| How to Cite this Article |
| Pubmed Style Ferrari C, Cola V, Magagnoli I, Costantini G, Ciammaichella L, Joechler M, Gandini G, Pisoni L. Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Vet. J.. 2026; 16(1): 724-730. doi:10.5455/OVJ.2026.v16.i1.68 Web Style Ferrari C, Cola V, Magagnoli I, Costantini G, Ciammaichella L, Joechler M, Gandini G, Pisoni L. Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. https://www.openveterinaryjournal.com/?mno=270861 [Access: February 04, 2026]. doi:10.5455/OVJ.2026.v16.i1.68 AMA (American Medical Association) Style Ferrari C, Cola V, Magagnoli I, Costantini G, Ciammaichella L, Joechler M, Gandini G, Pisoni L. Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Vet. J.. 2026; 16(1): 724-730. doi:10.5455/OVJ.2026.v16.i1.68 Vancouver/ICMJE Style Ferrari C, Cola V, Magagnoli I, Costantini G, Ciammaichella L, Joechler M, Gandini G, Pisoni L. Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Vet. J.. (2026), [cited February 04, 2026]; 16(1): 724-730. doi:10.5455/OVJ.2026.v16.i1.68 Harvard Style Ferrari, C., Cola, . V., Magagnoli, . I., Costantini, . G., Ciammaichella, . L., Joechler, . M., Gandini, . G. & Pisoni, . L. (2026) Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Vet. J., 16 (1), 724-730. doi:10.5455/OVJ.2026.v16.i1.68 Turabian Style Ferrari, Chiara, Veronica Cola, Ilaria Magagnoli, Gaia Costantini, Luca Ciammaichella, Monika Joechler, Gualtiero Gandini, and Luciano Pisoni. 2026. Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Veterinary Journal, 16 (1), 724-730. doi:10.5455/OVJ.2026.v16.i1.68 Chicago Style Ferrari, Chiara, Veronica Cola, Ilaria Magagnoli, Gaia Costantini, Luca Ciammaichella, Monika Joechler, Gualtiero Gandini, and Luciano Pisoni. "Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture." Open Veterinary Journal 16 (2026), 724-730. doi:10.5455/OVJ.2026.v16.i1.68 MLA (The Modern Language Association) Style Ferrari, Chiara, Veronica Cola, Ilaria Magagnoli, Gaia Costantini, Luca Ciammaichella, Monika Joechler, Gualtiero Gandini, and Luciano Pisoni. "Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture." Open Veterinary Journal 16.1 (2026), 724-730. Print. doi:10.5455/OVJ.2026.v16.i1.68 APA (American Psychological Association) Style Ferrari, C., Cola, . V., Magagnoli, . I., Costantini, . G., Ciammaichella, . L., Joechler, . M., Gandini, . G. & Pisoni, . L. (2026) Clinical features, diagnostic imaging findings, treatment, and outcome of a cat with C4 vertebral fracture and concomitant tracheal rupture. Open Veterinary Journal, 16 (1), 724-730. doi:10.5455/OVJ.2026.v16.i1.68 |

