




| Short Communication | ||
Open Vet. J.. 2025; 15(12): 6777-6785 Open Veterinary Journal, (2025), Vol. 15(12): 6777-6785 Short Communication Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary studyYutaro Ide1, Kent Yasunaga1 and Naoki Miura1,2*1Joint Graduate School of Veterinary Medicine, Kagoshima University, Kagoshima, Japan 2Veterinary Teaching Hospital, Joint Faculty of Veterinary Medicine, Kagoshima University, Kagoshima, Japan *Corresponding Author: Naoki Miura. Joint Graduate School of Veterinary Medicine, Kagoshima University, Kagoshima, Japan. Email: k9236024 [at] kadai.jp Submitted: 24/04/2025 Revised: 15/10/2025 Accepted: 02/11/2025 Published: 31/12/2025 © 2025 Open Veterinary Journal
AbstractBackground: Systemic hypertension in dogs requires timely diagnosis to prevent damage to the target organ. Although ultrasonographic assessment of the aorta-to-caudal vena cava (Ao/CVC) ratio has been proposed as a noninvasive indicator of elevated blood pressure, no studies have explored whether computed tomography (CT) can serve the same purpose. CT offers objective vascular measurements and may overcome some limitations of ultrasonography. Aim: This study aimed to determine whether CT-derived vascular ratios, specifically the Ao/CVC and a novel aorta-to-first lumbar vertebra (Ao/L1) ratio, differ between hypertensive and normotensive dogs. The influence of anesthetic status and measurement site on these ratios was also examined. Methods: In this retrospective study, 32 dogs that underwent same-day CT and Doppler Blood Pressure measurements were classified as hypertensive (systolic BP >140 mmHg) or normotensive. The abdominal aortic diameter was evaluated relative to the caudal vena cava and L1 vertebral body at three anatomical locations. Statistical comparisons were performed to assess differences between groups and potential confounding factors. Results: Neither the Ao/CVC nor the Ao/L1 ratio differed significantly between hypertensive and normotensive dogs (p=0.393 and p=0.229, respectively). However, the Ao/CVC ratio was significantly lower in anesthetized dogs (p=0.03), whereas the Ao/L1 ratio remained unaffected. No significant differences in the ratio values were observed between the measurement sites. These findings suggest that systemic hypertension does not induce measurable abdominal aortic enlargement, which is detectable by CT. Conclusion: This is the first study to evaluate CT-derived vascular indices as potential markers of systemic hypertension in dogs. The absence of significant differences shows that aortic diameter may not reliably reflect blood pressure status and that previous ultrasonographic findings may reflect venous variability or methodological artifacts rather than actual arterial changes. The Ao/L1 ratio may offer a stable, CT-specific metric for future vascular assessments. Prospective studies with direct modality comparisons are warranted. Keywords: Aorta to caudal vena cava ratio, Aorta to first lumbar vertebra ratio, Blood pressure, Canine, CT. IntroductionSystemic hypertension is generally defined as persistent systolic blood pressure (Acierno et al., 2018). In particular, secondary hypertension commands attention in veterinary medicine as it can be related to chronic kidney disease (Pérez-Sánchez et al., 2015), hyperadrenocorticism (García San José et al., 2024), and diabetes (Marynissen et al., 2016). However, in canine medicine, there is only one report on a determined abdominal aorta-caudal vena cava ratio as a potential index of systemic hypertension (Holland et al., 2020). Ultrasonography offers advantages such as simplicity and the ability to perform serial evaluations over time. However, it requires technical skills and is primarily limited to two-dimensional assessment within a restricted anatomical range. Computed tomography (CT) may offer some advantages over ultrasonography as an imaging modality for measuring vascular geometry. As an imaging modality, CT allows for objective evaluations. Because it is a whole-body imaging method, it is also a suitable method to ascertain the presence of diseases that may cause secondary hypertension or find complications of untreated hypertension, such as cerebral hemorrhage. Based on the advantages of CT and considering the report that the aorta to caudal vena cava ratio (Ao/CVC ratio) measured by ultrasound reflects systolic blood pressure, we retrospectively evaluated dogs that had undergone Doppler blood pressure and CT scans at our hospital to ascertain any differences in Ao/CVC ratio between hypertensive and normotensive dogs as the primary endpoint in this study. We also established a new parameter for assessing aortic dilation, i.e., the ratio of the abdominal aorta to the first lumbar vertebra (Ao/L1 ratio), to ensure that the evaluations were unaffected by dehydration. To the best of our knowledge, this is the first study to investigate whether CT can detect hypertension-associated changes in abdominal aortic diameter in dogs. We aimed to assess whether aortic dilatation previously observed by ultrasound could also be identified on CT and whether aortic diameter ratios—including a novel index based on the first lumbar vertebra (Ao/L1), which is known to exclude the effect of body weight—differ between hypertensive and normotensive dogs. This study also examined potential confounding factors such as measurement location and anesthetic status, providing a comprehensive evaluation of CT-based vascular assessment in dogs with systemic hypertension. Materials and MethodsStudy populationIn this retrospective and descriptive study, we evaluated data from 32 dogs that underwent CT examinations and blood pressure measurements on the same day while receiving medical care at Kagoshima University Veterinary Teaching Hospital (Kagoshima, Japan) between February and August 2024. The medical records of each dog were reviewed, and they were designated as hypertensive or normotensive dogs by an investigator (NM), a veterinarian affiliated with the Diagnostic Imaging Department of Kagoshima University Veterinary Teaching Hospital. Specifically, a dog was classified as normotensive when its systolic blood pressure was ≤140 mmHg or hypertensive when it exceeded 140 mmHg. Dogs with systolic blood pressure in the range of 140–159 mmHg, which is classified as the prehypertensive category in the American College of Veterinary Internal Medicine consensus statement (Acierno et al., 2018), were also included in the hypertensive group in this study, based on the assumption that sustained elevations in blood pressure could lead to changes in aortic diameter. This study excluded patients with vascular or spinal abnormalities or those with complex measurements (e.g., occupying lesions, positioning issues, or motion artifacts). Computed tomographyThe dogs underwent CT imaging with a dedicated 16-helical sliced CT scanner (Aquilion TSX-201A, Toshiba Medical Systems Corporation, Tochigi, Japan) with or without anesthesia. CT images were acquired using plain CT with a slice thickness of 0.5–1.0 mm, 120–135 kV, and 100–200 mAs, adjusted as necessary by the radiologist (NM) based on the patient’s weight. The anesthesia protocol was determined by the veterinarian, and it depended on the patient’s condition and temperament. A total of 20 dogs underwent CT scans without anesthesia, and 12 dogs were anesthetized for the procedure. The anesthetics used included combinations of propofol, dexmedetomidine, butorphanol, and isoflurane; specifically, 10 anesthetized dogs received propofol and isoflurane in 10 cases, and dexmedetomidine and butorphanol. Physical restraint was achieved in unanesthetized dogs using a box and towels as a simple restraint method. Imaging was performed without anesthesia only after confirming that the dog had accepted the restraint and was not experiencing excessive fear or discomfort. This method was not intended for complete immobilization but to reduce motion artifacts during imaging. Dogs underwent computed tomography in ventral recumbency in 31 cases and right lateral recumbency in one case. All images were acquired in the Digital Imaging and Communications in Medicine (DICOM) format and were read and measured using the OsiriX Ver. 5.9 DICOM viewer (Pixmeo, Bernex, Switzerland). Two investigators (YI and KY) performed all observations and measurements under the supervision of the other investigator and senior veterinarian (NM). Measurements were fully blinded between observers, and evaluation slice standardization was not implemented. Blood pressure measurementBlood pressure was measured 3–5 times by experienced veterinarians and/or veterinary nurses using the Doppler method, with outliers excluded, and the mean of the three measurements was taken as the adopted value. The measurements were taken 20 minutes after the patient arrived at the hospital, when the patient was confirmed to be calm. These were taken at the same time as a general physical examination and before the CT scan, while the patient was not anesthetized. When the animal appeared agitated at the time of measurement, this was recorded in its medical record. Blood pressure monitoring during is excluded from the standard protocol at KUVTH and was performed only in cases where the attending veterinarian and the radiologist deemed it necessary. No patients in the study population experienced severe hypotension during imaging. Measurement and evaluation of imagingCT images were typically reviewed and measured in the soft tissue condition, window level (WL) 50, and window width (WW) 350, with the WL and WW adjusted as necessary. The dilation of the abdominal aorta was assessed by the ratio of its diameter to the diameter of the caudal vena cava or the first lumbar vertebra (L1). The L1 diameter was selected as an indicator because it has been used in previous studies as a reference value that reflects body size and is not influenced by any cardiovascular anomalies, and its location on the thoracolumbar junction makes it readily identifiable and measurable on axial images (Swepson et al., 2022). We targeted three abdominal sites to measure the diameters of the adjacent aorta and caudal vena (Fig. 1A–E).
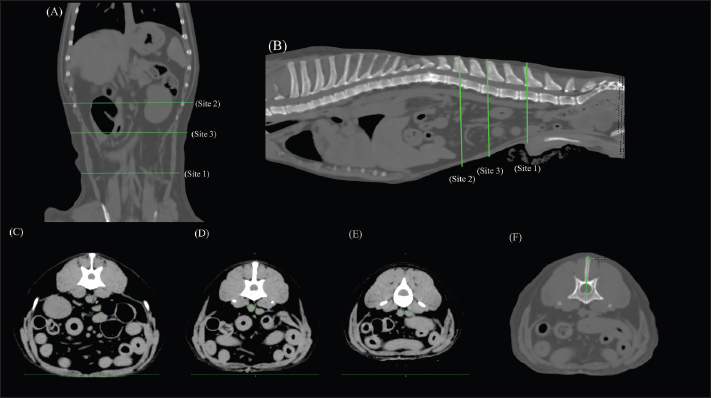
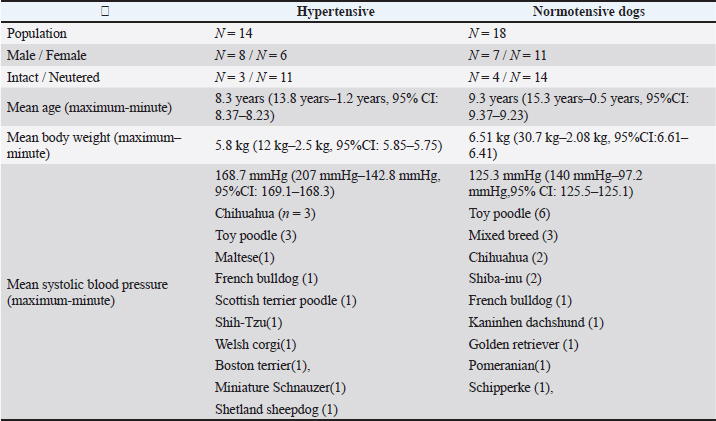
Fig. 1. Aorta, caudal vena cava, and first lumbar vertebra diameter measurements with computed tomography. Three anatomical sites targeted for the measurement of the diameters of the aorta and caudal vena cava in the abdomen are shown in dorsal (A) and sagittal views (B), with Site 1 at a well-defined location in the abdomen cranial to the origin of the bifurcated external iliac artery (C), Site 2 just below the first lumbar vertebra (L1) (E), and Site 3 at a medial point between Sites 1 and 2 and separated by at least five slices from them (D). The conditions for this image were soft tissue conditions, window level (WL): 50 and window width (WW): 300, slice thickness 1 mm. The diameter of the L1 vertebra (F) was measured as a straight line from the longest part of the spinous process to the ventral side of the vertebral body, where it can be clearly observed. The conditions for this image involved a bone window (WL: 300WW: 1,500, slice thickness 1 mm). Figure 1A and 1B illustrates the anatomical locations at which vascular measurements were performed. Measurements were conducted on slices in which the vessels exhibited a circular cross-sectional appearance. The first location (Site 1) was selected for the measurement site, determined in a similar report on ultrasonographic measurements (Holland et al., 2020), cranial to the origin of the bifurcated external iliac anatomy. Blood vessel diameters were measured again in the same manner at two different locations in the same region (Sites 2 and 3) to facilitate analytical checks for any error arising from a change in measurement site. Site 2 was selected at a cranial point along the abdominal blood vessels as a site same slice used for measuring the L1 vertebra, and Site 3 was selected as a midpoint between Sites 1 and 2. The midpoint is defined as a location separated by at least five slices from both Sites 1 and 2, based on the bifurcation of the renal artery, where there was little overlap or bifurcation of blood vessels. At each site, two perpendicular lines were drawn through the center of each blood vessel, extending to its border. The longest of the two lines was its maximal diameter, and its measured length was adopted as the evaluation value. The L1 diameter was measured as the maximum diameter from the vertebra to the spinous process (Fig. 1F). Statistical analysisData were analyzed using the statistical analysis software GraphPad Prism version 10.0.2 for Windows (GraphPad Software, www.graphpad.com). Data were compared between hypertensive and normotensive dogs, between males and females, and between anesthetized and unanesthetized dogs using Student’s t-test and paired t-test. Blood vessel diameters and diameter ratios were further compared between each of the three measurement sites using one-way ANOVA. Multiple comparisons between sites were performed using Tukey’s range test. A p value < 0.05 was considered statistically significant. Ethical approvalAs stated in this study, data were retrospectively collected from cases that required diagnostic examination, and no additional tests or invasive procedures were performed for research purposes. Therefore, ethical review was exempted, and there is no approval date or approval number. Results and DiscussionIn this study, we evaluated the association of abdominal aortic diameter measured by computed tomography with hypertension in dogs. The study population comprised 32 dogs (14 males and 18 females; mean age, 8.8 years; mean body weight, 6.18 kg), including 14 hypertensive and 18 normotensive individuals. Six dogs in each group underwent imaging under general anesthesia, while the remaining dogs were imaged without anesthesia. The hypertensive group (8 males and 6 females; mean age, 8.3 years; mean body weight, 5.8 kg) had a mean systolic blood pressure of 168.7 mmHg (median, 161 mmHg; range, 142.8–207 mmHg). This group included dogs with conditions known to predispose them to secondary hypertension—specifically, chronic kidney disease (n=2) and hyperadrenocorticism (n=1). Other diagnoses in this group included lung tumor (n=2), liver tumor (n=1), cervical disc herniation (n=1), bile duct cystadenoma (n=1), idiopathic epilepsy (n=1), perineal hernia (n=1), and cerebral hemorrhage (n=1); the etiology of the cerebral hemorrhage was not specified in the medical records. In contrast, the normotensive group (7 males and 11 females; mean age, 9.3 years; mean body weight, 6.51 kg) had a mean systolic pressure of 125.3 mmHg (range, 97.2–140 mmHg), and none of these dogs were diagnosed with secondary hypertension. No dogs in either group had been previously diagnosed with or treated for hypertension. Table 1 lists the clinical and demographic characteristics of the research population. Table 1. Clinical and demographic characteristics of hypertensive and normotensive dogs.
At measurement site 1, the hypertensive group exhibited a mean abdominal aortic diameter of 0.69 cm (range, 0.49–0.97 cm), a caudal vena cava diameter of 0.70 cm (0.42–1.09 cm), and an L1 vertebral body diameter of 2.78 cm (2.14–3.68 cm). In the normotensive group, the corresponding measurements were 0.73 cm (aorta), 0.69 cm (CVC), and 2.77 cm (L1). Table 2 presents detailed measurements for all three sites. Table 2. Blood vessel and L1 vertebral diameters in hypertensive and normotensive dogs.
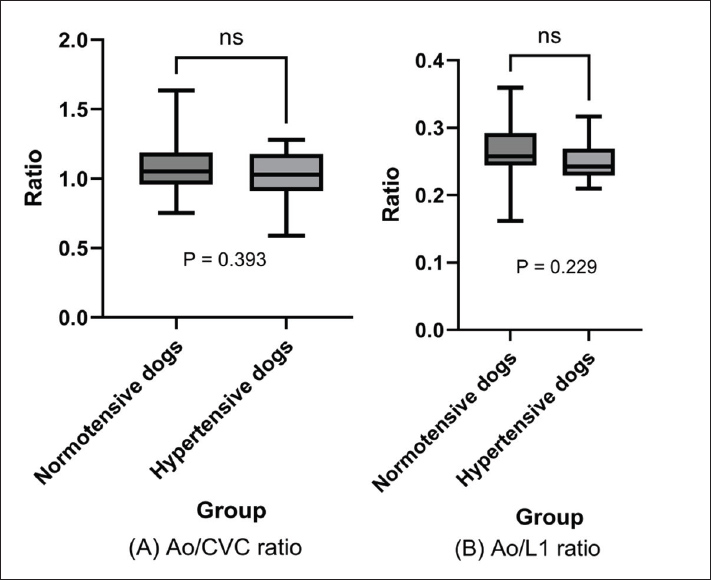
The primary endpoints of interest were Ao/CVC and Ao/L1 ratios. No statistically significant differences were found between hypertensive and normotensive dogs for either ratio (Ao/CVC: 1.03 ± 0.18 vs. 1.08 ± 0.20, p=0.393; Ao/L1: 0.250 ± 0.028 vs. 0.266 ± 0.041, p=0.229; Fig. 2A and B). These findings contrast with those of a previous study using ultrasonography, which concluded that the Ao/CVC ratio may indicate elevated blood pressure (Holland et al., 2020).
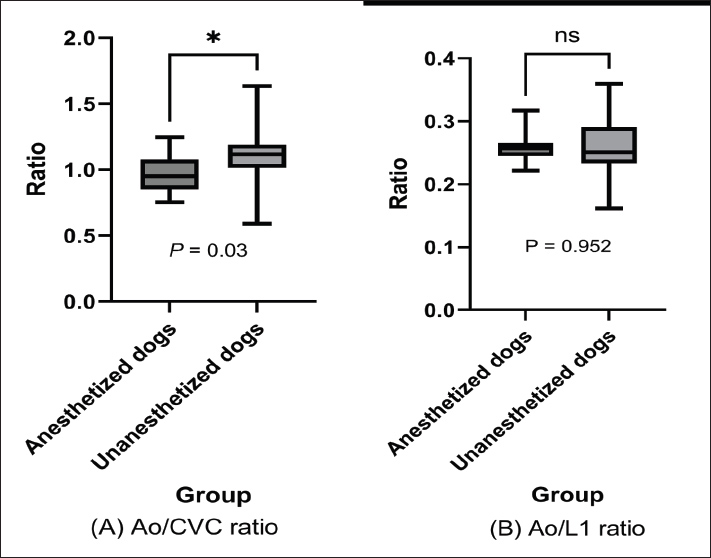
Fig. 2. Ao/CVC and Ao/L1 ratios: Hypertensive versus Normotensive dogs. The mean Ao/CVC and Ao/L1 ratios in hypertensive and normotensive dogs are represented in box plots, and no significant difference was observed between these population groups (Ao/CVC ratio: p=0.393; Ao/L1 ratio: p=0.229 > 0.05; t-test). In this study, the Ao/L1 ratio was proposed as an alternative indicator of aortic dilation, as it is less susceptible to changes in hydration status, unlike the CVC diameter. CVC is influenced by hydration status (Darnis et al., 2018; Herreriaal., 2020; Combet-Curt et al., 2023). Therefore, using vertebral body length as a reference may provide a more stable and reliable assessment of vascular size, representing a significant advantage of CT-based imaging. Concerning anesthesia, a significant difference was found in the Ao/CVC ratio between anesthetized and non-anesthetized dogs (p=0.03), while the Ao/L1 ratio remained unaffected (p=0.95; Fig. 3). This finding suggests that anesthetic agents may induce hypotension and consequent CVC dilation, reducing the Ao/CVC ratio (Lin et al., 2016; Hanazono et al., 2022; Sankisov and Newsom, 2024). In contrast, the Ao/L1 ratio demonstrated stability regardless of the anesthetic status, supporting its robustness as a measurement index. No statistically significant differences were observed in the subgroup analysis in which the dogs were classified into four groups based on anesthetic status and blood pressure (Supplemental Fig. 1). In two cases in this study population, the dogs had undergone sedation with dexmedetomidine, a drug that may affect vascular diameter. However, neither dog showed outlier values (respective Ao/CVC and Ao/L1 ratios of 0.986 and 0.31 in one case and 1.24 and 0.30 in the other), suggesting that the vascular effects of dexmedetomidine may have been minimal in these cases. Based on the vascular effects of anesthetic agents and these results, we believe that anesthesia-induced transient blood pressure fluctuations are unlikely to have a significant impact on aortic diameter.
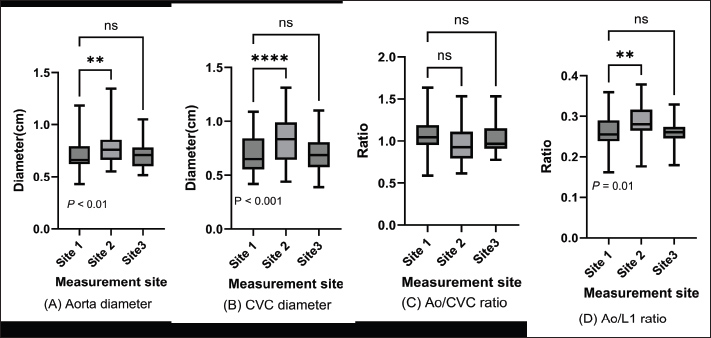
Fig. 3. Ao/CVC and Ao/L1 ratios in anesthetized and unanesthetized dogs. The mean Ao/CVC and Ao/L1 ratios in anesthetized dogs versus unanesthetized dogs are represented in box plots. The Ao/CVC ratio showed a significant difference (p=0.03) (A), but the Ao/L1 ratio did not (p=0.952 > 0.05) (B); t-test. The vascular diameters were also compared across the three measurement sites (Fig. 1A and B). Significant differences in aortic and CVC diameters were observed between Sites 1 and 2; however, no significant differences in Ao/CVC and Ao/L1 ratios were found at Site 3 or at any of the sites (Fig. 4), suggesting that measurement site has minimal impact on ratio-based assessments.
Fig. 4. Blood vessel diameters and Ao/CVC ratio by measurement site. Abdominal aorta and caudal vena cava diameters and Ao/CVC and Ao/L1 ratios are displayed in box plots for caudal, medial, and cranial measurement sites. One-way ANOVA indicated some significant differences between measurements (p < 0.05). Interestingly, the absence of significant differences in aortic diameter ratios between hypertensive and normotensive dogs observed in our CT-based study challenges the findings of a previous ultrasonographic report. Although the Ao/CVC ratio was proposed as a surrogate index of systemic hypertension in that study, the underlying physiological rationale for aortic dilation in response to hypertension, particularly in dogs, remains unclear. In humans, essential hypertension is the most common form (Vallée et al., 2019), whereas secondary hypertension predominates in veterinary patients. Chronic systemic hypertension is more likely to cause arterial wall remodeling, such as thickening and reduced compliance, than to induce substantial luminal expansion. Furthermore, the elevated Ao/CVC ratios observed in ultrasonography may be influenced by factors unrelated to aortic geometry, such as caudal vena cava collapse due to dehydration, increased sympathetic tone, or operator-dependent vessel compression during scanning. These factors are particularly relevant in ultrasonography, where probe pressure and respiratory phase can significantly affect vascular measurements (Muller et al., 2012; Bracco et al., 2025). In contrast, CT offers standardized and reproducible imaging with minimal operator dependence, potentially providing a more accurate anatomical representation. Therefore, our findings suggest that the previously reported association between hypertension and increased Ao/CVC ratios in ultrasound may not reflect actual aortic enlargement but rather variability in venous diameter or measurement artifacts. This study has several limitations. One limitation is the relatively small sample size. However, the inability to detect changes in aortic diameter between the two groups with clinically different blood pressure provides valuable insights into the relationship between blood pressure and the abdominal aorta. Furthermore, this study offers essential findings when comparing two groups with varying blood pressures using CT, such as the effects of the measurement site or the anesthetized state. Another significant limitation of this study is that vessel diameters were measured exclusively with CT, without simultaneous ultrasonography measurements. This limitation arises from the retrospective nature of the study, and future cohort studies should focus on comparing two different imaging modalities. ConclusionIn contrast to the previous ultrasound report, we found that the abdominal aortic diameter measured by CT does not appear to be changed by systemic hypertension. These results, combined with the known pathophysiological characteristics of chronic hypertension, indicate that systemic blood pressure may not exert a measurable effect on abdominal aortic diameter in dogs. In this context, using CT as a diagnostic modality may offer advantages in anatomical accuracy. However, it may also reveal that aortic geometry is not a reliable indicator of hypertension in the absence of vascular disease. There is a need for large-scale, prospective studies with simultaneous CT and ultrasonographic measurements to elucidate any potential actual utility or lack of utility of these imaging modalities for blood pressure assessments. Therefore, our study challenges the physiological assumptions underlying the use of vascular ratios in hypertensive screening and underscores the importance of integrating multiple modalities and clinical parameters for accurate blood pressure assessment in veterinary patients. AcknowledgmentsWe thank all our colleagues at Kagoshima University Veterinary Teaching Hospital for their help in collecting CT images and providing medical care to our patients, our fellow researcher, Nobuhiro Nozaki, for helping with statistical analysis, and Henry Smith (Co-chair of the Veterinary Special Interest Group in the European Medical Writers Association) for helping with the English editing of a draft of the manuscript. Conflict of interestThe authors have no competing interests to declare. FundingThis study received no external funding. Author contributionsAll authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yutaro Ide, Kent Yasunaga, and Naoki Miura. Yutaro Ide wrote the first draft of the manuscript, and all authors commented on previous versions of the manuscript. All authors have read and approved the final version of the manuscript. Data availabilityThe authors will make available the raw data supporting the conclusions of this article on request. ReferencesAcierno, M.J., Brown, S., Coleman, A.E., Jepson, R.E., Papich, M., Stepien, R.L. and Syme, H.M. 2018. ACVIM consensus statement: guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J. Vet. Internal. Med. 32(6), 1803–1822; doi: 10.1111/jvim.15331 Bracco, M.I., Yousefi, A.A.K., Rouet, L. and Avril, S. 2025. Ultrasound Probe Pressure Affects Aortic Wall Stiffness: a Patient-Specific Computational Study in Abdominal Aortic Aneurysms. Ann. Biomed. Eng. 53(1), 71–82; doi:10.1007/s10439-024-03608-8 Combet-Curt, J., Pouzot-Nevoret, C., Cambournac, M., Magnin, M., Nectoux, A., Bonnet-Garin, J.M., Goy-Thollot, I. and Barthélemy, A. 2023. Ultrasonographic measurement of caudal vena cava to aorta ratio during fluid resuscitation of dogs with spontaneous circulatory shock. J. Small Anim. Pract. 64(11), 669–679; doi:10.1111/jsap.13654 Darnis, E., Boysen, S., Merveille, A.C., Desquilbet, L., Chalhoub, S. and Gommeren, K. 2018. Establishment of reference values of the caudal vena cava by fast-ultrasonography through different views in healthy dogs. J. Vet. Internal. Med. 32(4), 1308–1318; doi:10.1111/jvim.15136 García San José, P., Pérez-Alenza, M.D., Alonso-Miguel, D., González Sanz, S. and Arenas Bermejo, C. 2024. Prevalence of systemic hypertension and control of systolic blood pressure in a cohort of 14 dogs with adrenal-dependent hypercortisolism during the first year of trilostane treatment or after adrenalectomy. Animals Open. Access. J. From. MDPI. 14(3), 511; doi:10.3390/ani14030511 Hanazono, K., Nakamoto, M., Hori, A., Miyoshi, K., Nakade, T., Itami, T., Sano, T., Kato, K., Ito, A., Tanaka, K., Yamashita, K. and Endoh, D. 2022. Evaluation of caudal vena cava size using computed tomography in dogs under general anesthesia. J. Vet. Med. Sci. 84(12), 1556–1562; doi:10.1292/jvms.22-0122 Herreria-Bustillo, V.J., Fitzgerald, E. and Humm, K.R. 2019. Caval-aortic ratio and caudal vena cava diameter in dogs before and after blood donation. J. Vet. Emergency. Crit. Care. (San. Antonio. Tex. 2001). 29(6), 643–646; doi:10.1111/vec.12900 Holland, M., Hudson, J., Bao, Y. and Gaillard, P. 2020. Aortic to caudal vena cava ratio measurements using abdominal ultrasound are increased in dogs with confirmed systemic hypertension. Vet. Radiol. &. Ultrasound. 61(2), 206–214; doi:10.1111/vru.12822 Lin, E.E., Chen, A.E., Panebianco, N., Conlon, T., Ju, N.R., Carlson, D., Kopenitz, J. and Nishisaki, A. 2016. Effect of Inhalational Anesthetics and Positive-pressure Ventilation on Ultrasound Assessment of the Great Vessels: a Prospective Study at a Children's Hospital. Anesthesiology 124(4), 870–877; doi:10.1097/ALN.0000000000001032 Marynissen, S.J.J., Smets, P.M.Y., Ghys, L.F.E., Paepe, D., Delanghe, J., Galac, S., Meyer, E., Lefebvre, H.P. and Daminet, S. 2016. Long-term follow-up of renal function assessing serum cystatin C in dogs with diabetes mellitus or hyperadrenocorticism. Vet. Clin. Pathol. 45(2), 320–329; doi:10.1111/vcp.12365 Muller, L., Bobbia, X., Toumi, M., Louart, G., Molinari, N., Ragonnet, B., Quintard, H., Leone, M., Zoric, L. and Lefrant, J.Y. 2012. Respiratory variations of inferior vena cava diameter to predict fluid responsiveness in spontaneously breathing patients with acute circulatory failure: need for a cautious use. Crit. Care (London. England). 16(5), R188; doi:10.1186/cc11672 Pérez-Sánchez, A.P., Del-Angel-Caraza, J., Quijano-Hernández, I.A. and Barbosa-Mireles, M.A. 2015. Obesity-hypertension and its relation to other diseases in dogs. Vet. Res. Commun. 39(1), 45–51; doi:10.1007/s11259-015-9630-9 Rabozzi, R., Oricco, S., Meneghini, C., Bucci, M. and Franci, P. 2020. Evaluation of the caudal vena cava diameter to abdominal aortic diameter ratio and the caudal vena cava respiratory collapsibility for predicting fluid responsiveness in a heterogeneous population of hospitalized conscious dogs. J. Vet. Med. Sci. 82(3), 337–344; doi:10.1292/jvms.19-0028 Sankisov, J.N. and Newsom, L. 2024. Computed tomographic reference ranges of intrathoracic caudal vena cava ratios in sedated adult dogs without cardiac, pulmonary, or hypovolemic disease. Vet. Med. Sci. 10(4), e1510; doi:10.1002/vms3.1510 Swepson, R., Hosgood, G. and Stander, N. 2022. Algorithmic estimation of adrenal volume based on bodyweight and CT landmarks in dogs. Vet. Radiol. Ultrasound 63, 264–271; doi:10.1111/vru.13047 Vallée, A., Safar, M.E. and Blacher, J. 2019. Hypertension artérielle permanente essentielle : définitions et revue hémodynamique, clinique et thérapeutique Essential hypertension: Definitions, hemodynamic, clinical and therapeutic review. Presse. Medicale. (Paris. France. 1983). 48(1 Pt 1), 19–28; doi:10.1016/j.lpm.2018.11.017 Supplementary Material
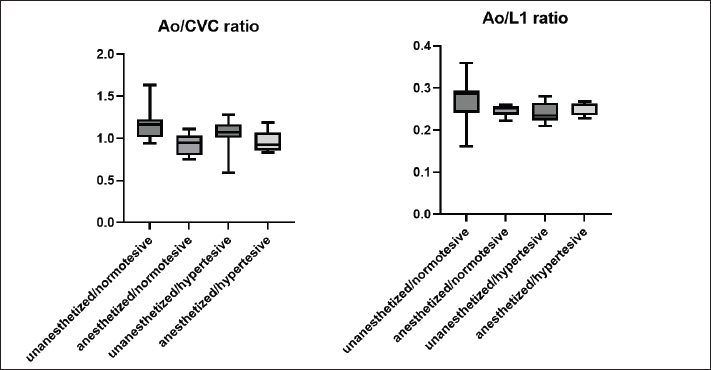
Supplemental Fig. 1. Comparison of Ao/CVC and Ao/L1 ratios among subgroups classified based on anesthetic status and blood pressure. The Ao/CVC and Ao/L1 ratios were compared among the four groups categorized by anesthesia status (anesthetized or unanesthetized) and blood pressure (hypertensive or normotensive). As determined by one-way ANOVA, no significant differences were observed. | ||

| How to Cite this Article |
| Pubmed Style Ide Y, Yasunaga K, Miura N. Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Vet. J.. 2025; 15(12): 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 Web Style Ide Y, Yasunaga K, Miura N. Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. https://www.openveterinaryjournal.com/?mno=254110 [Access: June 26, 2026]. doi:10.5455/OVJ.2025.v15.i12.56 AMA (American Medical Association) Style Ide Y, Yasunaga K, Miura N. Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Vet. J.. 2025; 15(12): 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 Vancouver/ICMJE Style Ide Y, Yasunaga K, Miura N. Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Vet. J.. (2025), [cited June 26, 2026]; 15(12): 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 Harvard Style Ide, Y., Yasunaga, . K. & Miura, . N. (2025) Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Vet. J., 15 (12), 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 Turabian Style Ide, Yutaro, Kent Yasunaga, and Naoki Miura. 2025. Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Veterinary Journal, 15 (12), 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 Chicago Style Ide, Yutaro, Kent Yasunaga, and Naoki Miura. "Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study." Open Veterinary Journal 15 (2025), 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 MLA (The Modern Language Association) Style Ide, Yutaro, Kent Yasunaga, and Naoki Miura. "Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study." Open Veterinary Journal 15.12 (2025), 6777-6785. Print. doi:10.5455/OVJ.2025.v15.i12.56 APA (American Psychological Association) Style Ide, Y., Yasunaga, . K. & Miura, . N. (2025) Computed tomographic assessment of abdominal aortic diameter is not associated with systemic hypertension in dogs: A preliminary study. Open Veterinary Journal, 15 (12), 6777-6785. doi:10.5455/OVJ.2025.v15.i12.56 |

