




| Research Article | ||
Open Vet. J.. 2026; 16(5): 2610-2618 Open Veterinary Journal, (2026), Vol. 16(5): 2610-2618 Research Article Effect of desmopressin on buccal mucosal bleeding time in healthy dogsShuji Suzuki*, Sachiyo Tanaka, Nobuo Kanno, Takuya Yogo, Yasuji Harada and Yasushi HaraLaboratory of Veterinary Surgery, Nippon Veterinary and Life Science University, Tokyo, Japan *Corresponding Author: Shuji Suzuki. Laboratory of Veterinary Surgery, Nippon Veterinary and Life Science University, Tokyo, Japan. Email: shujisuzuki [at] nvlu.ac.jp Submitted: 02/02/2026 Revised: 04/04/2026 Accepted: 11/04/2026 Published: 31/05/2026 © 2025 Open Veterinary Journal
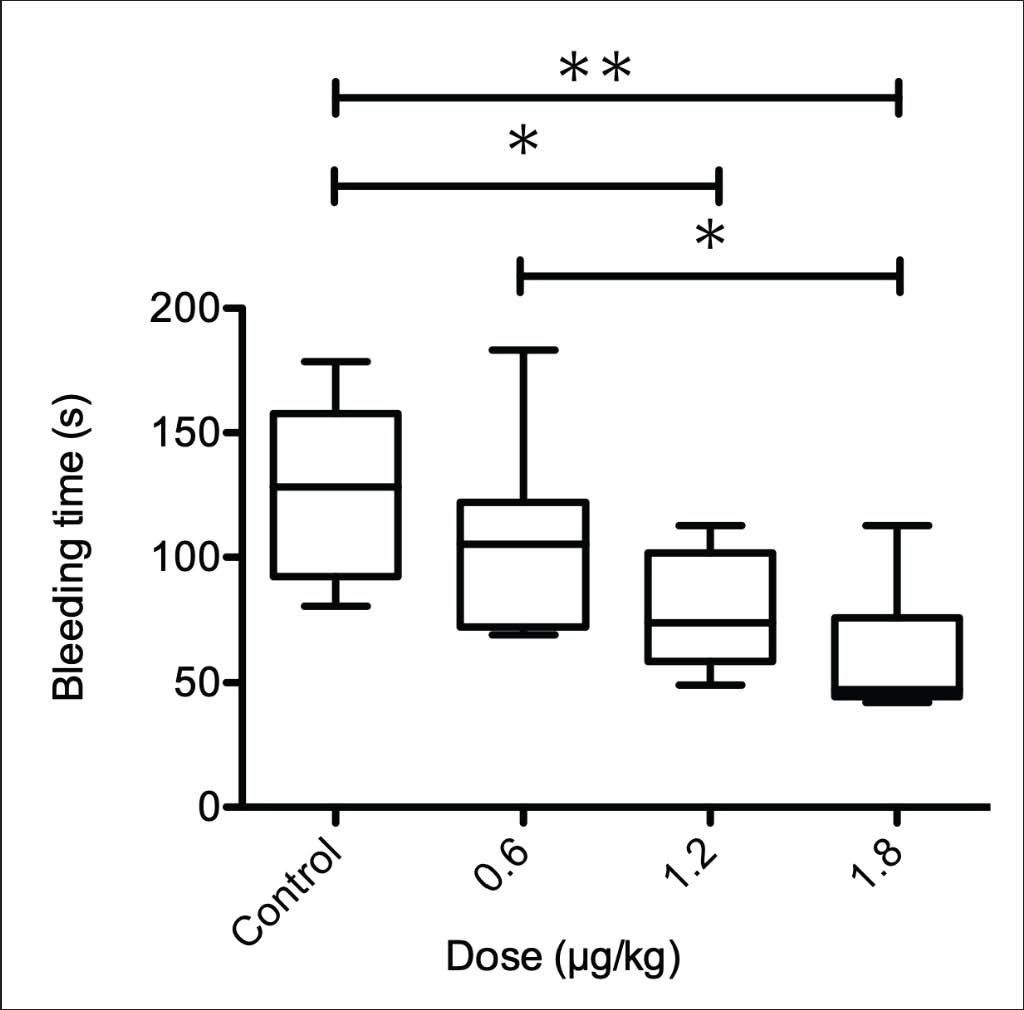
AbstractBackground: Desmopressin acetate (DDAVP) is used as a hemostatic adjunct because it can improve primary hemostasis and increase Factor VIII- and von Willebrand factor-related variables. However, its effects in dogs under general anesthesia are not well defined. Aim: This study aimed to evaluate the effect of DDAVP on buccal mucosal bleeding time (BMBT) in anesthetized healthy dogs and to assess concurrent changes in plasma FVIII antigen (FVIII:Ag). Methods: Twenty-seven healthy Beagle dogs were randomly assigned to receive intravenous saline (control; n=8) or DDAVP at 0.6 (n=7), 1.2 (n=6), or 1.8 µg/kg (n=6) under isoflurane anesthesia. The BMBT was measured 30 minutes after administration. Blood samples were collected at baseline and at 30 and 60 minutes to measure FVIII:Ag, complete blood count, prothrombin time, activated partial thromboplastin time, fibrinogen, and electrolytes. Heart rate and arterial blood pressure were recorded at the same time points. Results: At 30 minutes after administration, the BMBT values were 128.2 (92.1–157.7) seconds in the control group, 105.2 (72.4–122.0) seconds in the 0.6 µg/kg group, 74.1 (58.6–101.8) seconds in the 1.2 µg/kg group, and 47.2 (44.4–76.1) seconds in the 1.8 µg/kg group. BMBT was significantly shorter in the 1.2 and 1.8 µg/kg groups than in the controls, and in the 1.8 µg/kg group than in the 0.6 µg/kg group (p < 0.05). FVIII:Ag levels at 60 minutes were significantly higher in the 1.8 µg/kg group than in the control group (p < 0.05) and increased from baseline to 60 minutes in the 1.2 and 1.8 µg/kg groups (p < 0.05). No other significant differences were detected. Conclusion: DDAVP dose-dependently shortened BMBT and increased FVIII:Ag in 60 minutes in healthy anesthetized dogs. These findings provide preliminary data and support further investigation of DDAVP in patients undergoing surgery. Keywords: Buccal mucosal bleeding time, Desmopressin, Dog, Factor VIII antigen, Primary hemostasis. IntroductionFactor VIII (FVIII) is a plasma glycoprotein that circulates in a noncovalent complex with von Willebrand factor (vWF). FVIII antigen (FVIII:Ag) reflects the circulating FVIII protein level, whereas FVIII coagulant activity (FVIII:C) plays a pivotal role in thrombin generation and fibrin clot formation (Hoyer, 1981; Bowie, 1984; Chavin, 1984). vWF, which is synthesized by vascular endothelial cells and megakaryocytes, mediates platelet adhesion to the injured vessel wall and stabilizes FVIII in the circulation. Desmopressin acetate (DDAVP; 1-deamino-8-D-arginine vasopressin) is a synthetic vasopressin analog that can improve primary hemostasis and increase circulating FVIII- and vWF-related variables. It has been investigated as a hemostatic adjunct. In normal dogs, DDAVP administration alters hemostatic parameters, including FVIII and vWF levels (Johnstone and Crane, 1986). In humans, DDAVP has been evaluated as a blood-sparing strategy in cardiac surgery. A randomized trial reported reduced blood loss after cardiac surgery with DDAVP administration (Salzman et al., 1986); however, another trial did not demonstrate a reduction in blood loss in uncomplicated cardiac surgery (Hackmann et al., 1989), indicating that clinical effects may vary by patient population and surgical context. Perioperative bleeding during major surgery is multifactorial and can involve impairment of primary hemostasis and changes in coagulation and fibrinolysis. Studies in patients undergoing extracorporeal circulation have described hemostatic derangements, including alterations in plasma coagulation factors, fibrinolysis activation, and platelet activation and dysfunction (Bachmann et al., 1975; McKenna et al., 1975; Umlas, 1976; Desborough et al., 2017; Picchio et al., 2025). Evidence regarding the hemostatic effects of DDAVP in dogs remains limited, particularly under general anesthesia and in perioperative settings, where improvement of primary hemostasis may be clinically relevant. Therefore, this study evaluated the effect of DDAVP on primary hemostasis in anesthetized healthy dogs using buccal mucosal bleeding time (BMBT) as a clinical screening test. Materials and MethodsAnimalsA total of 27 healthy Beagle dogs were used, including 14 males (mean body weight, 10.1 kg; range, 7.0–13.0 kg; mean age, 20 months; range, 17–32 months) and 13 females (mean body weight, 9.2 kg; range, 8.0–11.0 kg; mean age, 17.7 months; range, 12–38 months). Study design and experimental protocolDogs were randomly assigned to four groups: a control group (six males, two females; n=8), a DDAVP 0.6 µg/kg group (three males, four females; n=7), a DDAVP 1.2 µg/kg group (two males, four females; n=6), and a DDAVP 1.8 µg/kg group (three males, three females; n=6). Dogs were randomly allocated to the control or DDAVP groups using a random number table generated by Takuya Yogo. Study solutions were prepared by Sachiyo Tanaka according to the allocation list and administered intravenously (IV) by Nobuo Kanno. BMBT was measured by Shuji Suzuki. Under general anesthesia, the control group received 15 ml of sterile saline IV as a single bolus injection. The treatment groups received DDAVP injection (DDAVP; desmopressin; Kyowa Kirin Co., Ltd., Tokyo, Japan) at 0.6, 1.2, or 1.8 µg/kg IV. In all DDAVP groups, the dose was diluted with sterile saline to a total volume of 15 ml and administered as a single IV bolus injection. In a prior dose–response study in normal dogs (0.2–0.6 µg/kg IV), FVIII–related parameters increased in a dose-dependent manner and peaked at 30–60 minutes. Because dogs require relatively higher doses than humans to achieve comparable responses, we selected 0.6 µg/kg (the highest dose evaluated in that report) as the lowest dose in the present study to ensure a measurable biological effect (Johnstone and Crane, 1986). Higher doses (1.2 and 1.8 µg/kg) were then explored to assess a broader dose–response range, with 1.8 µg/kg selected as a pragmatic upper dose that remained feasible for single intravenous bolus administration under controlled anesthetic monitoring. Premedication consisted of medetomidine (Orion Corporation, Espoo, Finland) at 20 µg/kg and butorphanol (Meiji Seika Pharma Co., Ltd., Tokyo, Japan) at 0.1 mg/kg administered intramuscularly. Anesthesia was induced with 6 mg/kg IV propofol (Fresenius Kabi Japan K.K., Tokyo, Japan), followed by endotracheal intubation. Anesthesia was maintained with isoflurane (Mylan Seiyaku Ltd., Tokyo, Japan). Lactated Ringer’s solution (5 ml/kg/h) was administered throughout anesthesia. Dogs were mechanically ventilated with 100% oxygen using volume-controlled ventilation at a respiratory rate of 10 breaths/min and a target tidal volume of approximately 10–15 ml/kg. The heart rate (HR) and non-invasive arterial blood pressure were monitored using an oscillometric device with the cuff placed on the tail. The end-tidal CO₂ and SpO₂ were continuously monitored during anesthesia. The body temperature was monitored and maintained at ≥37.0°C. After approximately 30 minutes of anesthetic maintenance and confirmation of stable monitored parameters, baseline measurements were obtained. HR, systolic arterial pressure (SAP), mean arterial pressure (MAP), and diastolic arterial pressure (DAP) were recorded, and blood samples were collected immediately before saline or DDAVP (baseline) and at 30 and 60 minutes after administration. BMBT was measured at 30 minutes after treatment. After the completion of the experiment, dogs were allowed to recover from anesthesia and were monitored to confirm the absence of clinical abnormalities. Blood sampling and laboratory analysisBlood samples were collected from the jugular vein at baseline and at 30 and 60 minutes after administration using a 5-ml syringe (TOP Corporation, Tokyo, Japan) with a 22-gauge needle (TOP Corporation, Tokyo, Japan). Blood was dispensed into one ethylenediaminetetraacetic acid (EDTA) tube, one heparin tube, and two 3.13% sodium citrate tubes at each time point. EDTA-anticoagulated blood (Fujifilm, Tokyo, Japan) was used for complete blood count (CBC) analysis using an automated hematology analyzer (Nihon Kohden, Tokyo, Japan). Heparinized blood (Fujifilm, Tokyo, Japan) was centrifuged for 5 minutes, and a clinical chemistry analyzer (Fujifilm, Tokyo, Japan) was used to analyze plasma for electrolytes (K, Na, and Cl). Citrated blood samples (3.13% sodium citrate; Sekisui Medical Co., Ltd., Tokyo, Japan) were used to measure prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen, and FVIII:Ag. PT, APTT, and fibrinogen levels were measured at a commercial laboratory using standard clot-based assays with an optical clot detection method. For FVIII:Ag measurement, citrated plasma was separated by centrifugation at 1,500 × g for 10 minutes at room temperature (15°C–25°C), aliquoted, and stored at −80°C until analysis. The samples underwent a single freeze–thaw cycle. Buccal mucosal bleeding timeAt 30 minutes after administration of DDAVP or saline, BMBT was measured under general anesthesia. The upper lip was folded, and a bandage was wrapped around the maxilla to maintain positioning. A standardized mucosal incision was made on the buccal mucosa above the premolar teeth using an adult Surgicutt device with a 5-mm blade (International Technidyne Corp., Edison, NJ; catalog no. J0522S). Blood was gently blotted with dedicated filter paper every 3–4 seconds without contacting the incision site, and the time from incision until bleeding ceased was recorded as BMBT. Areas with visibly congested vessels were avoided. All BMBT measurements were performed by the same investigator, who was blinded to group allocation. The BMBT was assessed once, 30 minutes after saline or desmopressin administration, because previous work in normal dogs demonstrated a rapid increase in FVIII parameters after intravenous desmopressin, with peak responses occurring approximately 30–60 minutes post-infusion (Johnstone and Crane, 1986). A pre-treatment BMBT was not obtained to avoid a second mucosal incision during the same anesthetic session, which could itself affect subsequent bleeding time measurements. FVIII:Ag measurementPlasma FVIII:Ag concentration was measured using a commercially available canine sandwich enzyme-linked immunosorbent assay kit (Cosmo Bio Co., Ltd., Tokyo, Japan). According to the manufacturer, the assay is intended for antigen detection in plasma, with a detection range of 78–5,000 pg/ml and a sensitivity of <28 pg/ml. Manufacturer-reported performance characteristics include intra- and inter-assay coefficients of variation of < 10% and < 12%, respectively, and no significant cross-reactivity with related proteins. In sodium citrate plasma, recovery was 80%–97%, and dilution linearity was reported for serial dilutions (1:2 to 1:16), with observed-to-expected values of 79%–103%. Briefly, the standards, blank, and diluted samples (100 µl/well) were incubated at 37°C for 1 hour, followed by sequential incubation with detection reagents A and B at 37°C for 1 hour and 30 minutes, respectively, followed by washing according to the kit protocol. The 3,3',5,5'-tetramethylbenzidine substrate was added and incubated at 37°C for 10–20 minutes protected from light (not exceeding 30 minutes), stop solution was added, and absorbance was measured immediately at 450 nm using a microplate reader. Duplicate readings were averaged; a standard curve was generated using blank-corrected optical density values, and sample concentrations were calculated from the fitted curve. Plasma samples were diluted according to the manufacturer’s instructions to yield concentrations within the standard curve range. Statistical analysisStatistical analyses were performed using GraphPad Prism version 10.6.1 (GraphPad Software, Boston, MA). Because of the small sample size in each group (n=6–8) and non-normal distribution in several outcomes, data were summarized as median [interquartile range (IQR)], and nonparametric tests were used. Formal hypothesis testing focused on the primary endpoint (BMBT) to limit inflation of type I error due to multiple outcome measures; analyses of secondary and safety endpoints were considered exploratory and should be interpreted cautiously. The BMBT was prespecified as the primary endpoint. No formal a priori power calculation was performed because this was an exploratory study, and the sample size was determined by feasibility. For the primary endpoint, BMBT (measured once after 30 minutes), groups were compared using the Kruskal–Wallis test followed by Dunn’s multiple comparison test. For repeated-measures outcomes measured at baseline and at 30 and 60 minutes, the Friedman test followed by Dunn’s multiple comparison test was used to assess within-group changes over time. Between-group comparisons were performed at each time point using the Kruskal–Wallis test followed by Dunn’s multiple comparison test. A two-sided p value <0.05 was considered statistically significant. Ethical approvalThe relevant Laboratory Animal Committee approved this study (approval number: 2019J-29), and all dogs were handled in accordance with institutional guidelines for laboratory animals. ResultsBuccal mucosal bleeding timeData are presented as the median (IQR) unless otherwise stated. At 30 minutes after administration, the BMBT values were 128.2 (92.1–157.7) seconds in the control group, 105.2 (72.4–122.0) seconds in the 0.6 µg/kg group, 74.1 (58.6–101.8) seconds in the 1.2 µg/kg group, and 47.2 (44.4–76.1) seconds in the 1.8 µg/kg group. BMBT was significantly shorter in the 1.2 and 1.8 µg/kg groups than in the control group (p < 0.05) and in the 1.8 µg/kg group than in the 0.6 µg/kg group (p < 0.05; Fig. 1).
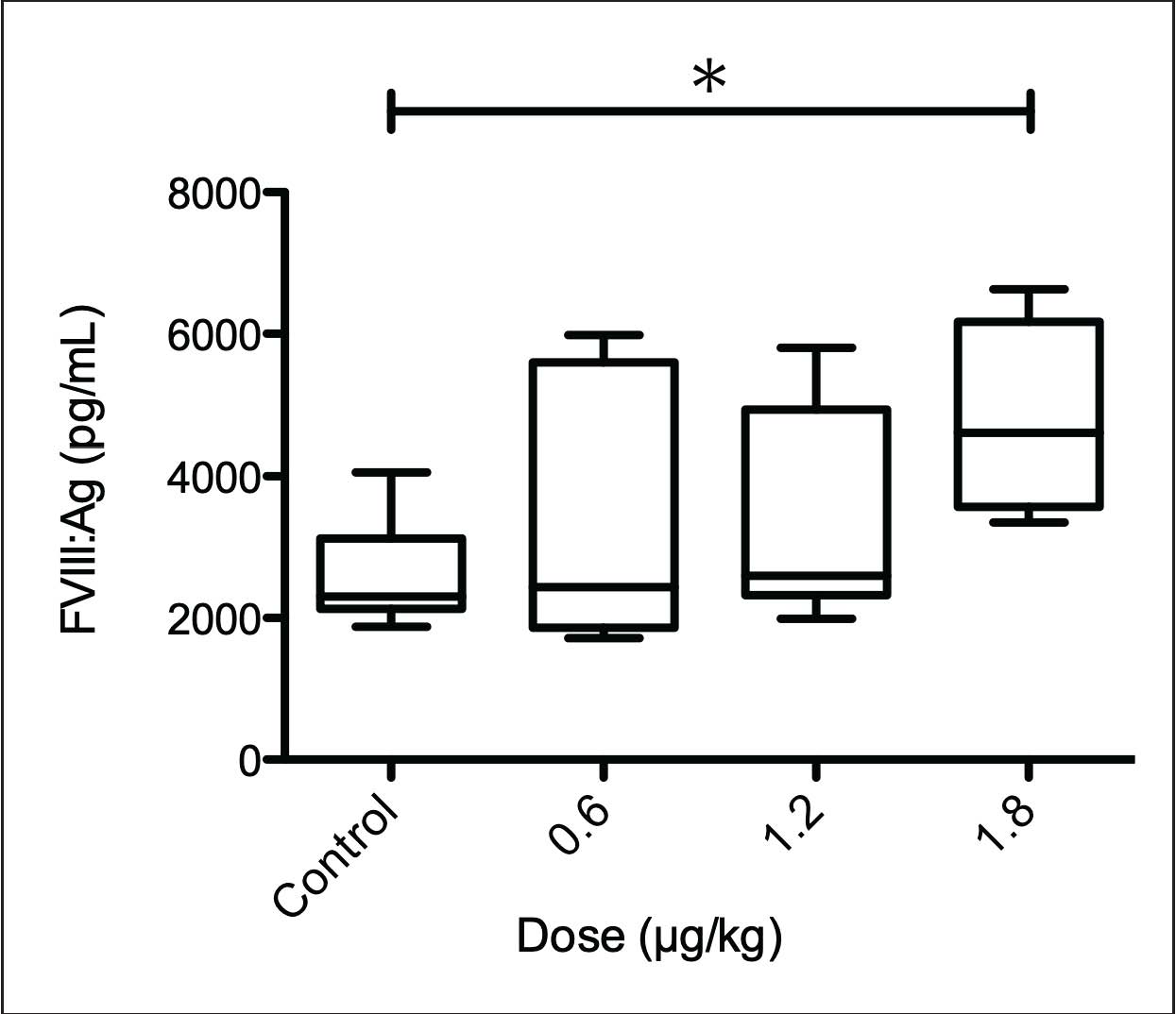
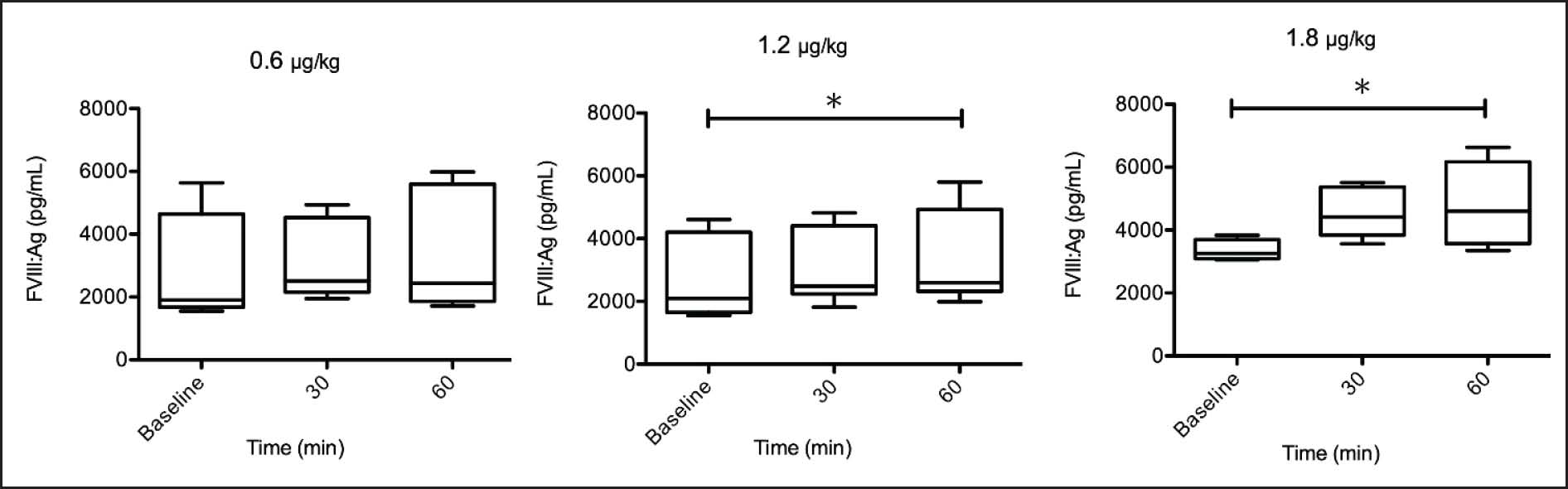
Fig. 1. BMBT measured 30 minutes after intravenous administration of saline (control; n=8) or (DDAVP; 0.6 µg/kg, n=7; 1.2 µg/kg, n=6; 1.8 µg/kg, n=6) in anesthetized healthy dogs. Box-and-whisker plots show the median (horizontal line), IQR (box; 25th–75th percentiles), and the 5th–95th percentiles (whiskers). Statistical comparisons were performed using the Kruskal–Wallis test followed by Dunn’s multiple comparison test. *p < 0.05, **p < 0.01 (between the indicated groups). FVIII antigenAt 60 minutes after administration, FVIII:Ag was significantly higher in the 1.8 µg/kg group than in the control group (p < 0.05; Fig. 2). In addition, FVIII:Ag increased significantly from baseline to 60 minutes in the 1.2 and 1.8 µg/kg groups (p < 0.05; Fig. 3).
Fig. 2. Plasma FVIII:Ag concentrations at 60 minutes after intravenous administration of saline (control; n=8) or (DDAVP; 0.6 µg/kg, n=7; 1.2 µg/kg, n=6; 1.8 µg/kg, n=6) in anesthetized healthy dogs. Box-and-whisker plots show the median (horizontal line), IQR (box; 25th–75th percentiles), and the 5th–95th percentiles (whiskers). Statistical comparisons were performed using the Kruskal–Wallis test followed by Dunn’s multiple comparison test. *p < 0.05 versus control at the same time point.
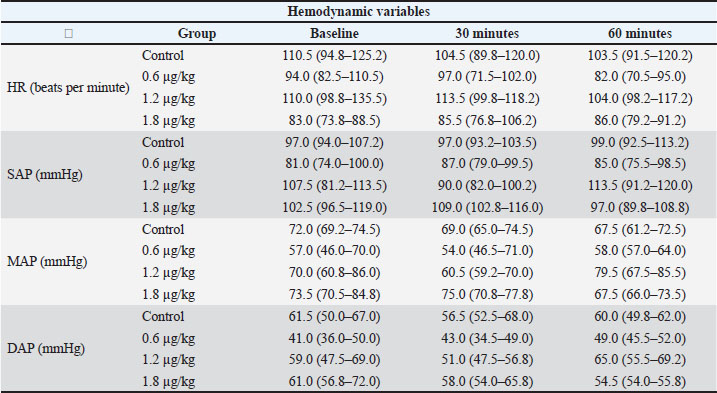
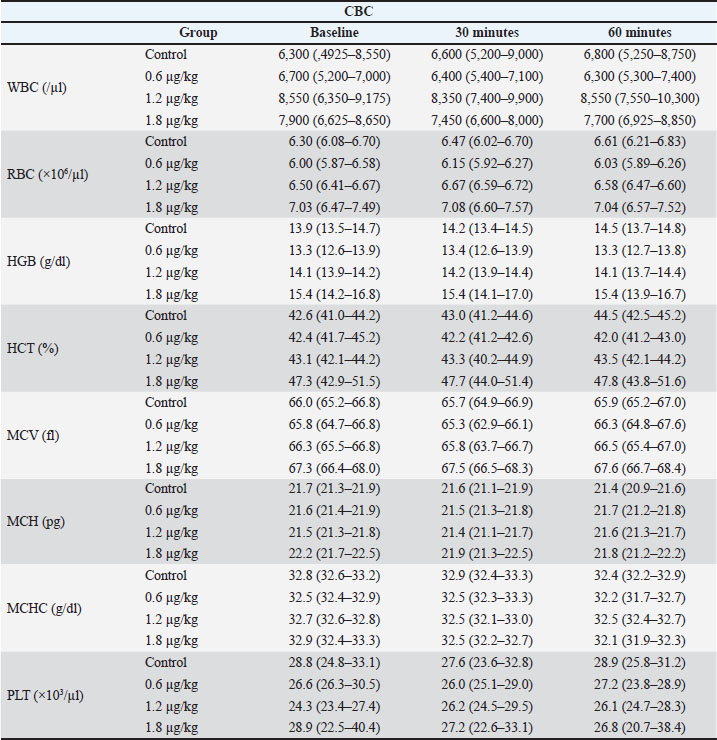
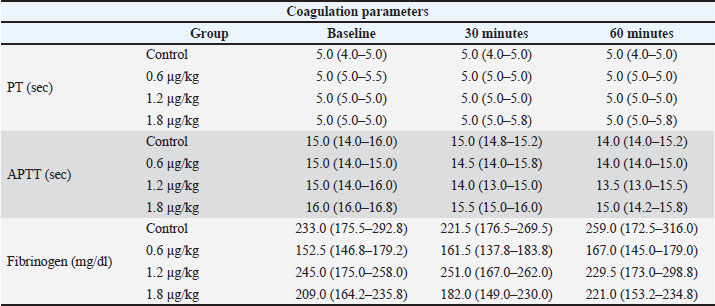
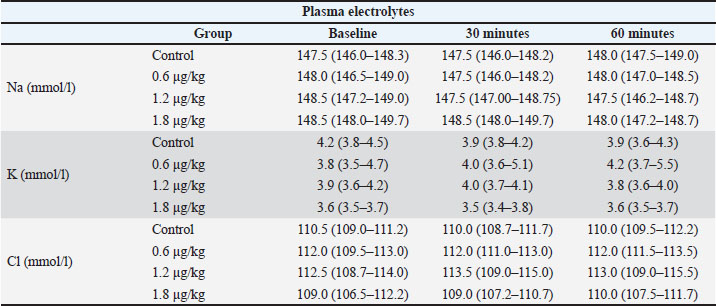
Fig. 3. Time-course changes in plasma FVIII:Ag concentrations after intravenous administration of DDAVP in anesthetized healthy dogs. FVIII:Ag was measured at baseline and at 30 and 60 minutes after administration. Panels show the DDAVP 0.6 µg/kg (n=7), 1.2 µg/kg (n=6), and 1.8 µg/kg (n=6) groups. Box-and-whisker plots show the median (horizontal line), IQR (box; 25th–75th percentiles), and the 5th–95th percentiles (whiskers). Changes over time (baseline, 30, and 60 minutes) within each DDAVP group were analyzed using the Friedman test followed by Dunn’s multiple comparison test. *p < 0.05 versus baseline within the same group. Other variables (HR, blood pressure, CBC, coagulation parameters, and electrolytes). HR, arterial blood pressure, CBC, PT, APTT, fibrinogen, and plasma electrolytes (Na, K, and Cl) were compared among the four groups at baseline, 30, and 60 minutes. No significant differences were detected (Tables 1–4). Table 1. Hemodynamic variables at baseline, 30, and 60 minutes after IV saline (Control) or DDAVP (0.6, 1.2, or 1.8 µg/kg) in anesthetized healthy dogs. Data are presented as median (IQR, 25th–75th percentiles).
Table 2. CBC variables at baseline, 30, and 60 minutes after IV saline (Control) or DDAVP (0.6, 1.2, or 1.8 µg/kg) in anesthetized healthy dogs. Data are presented as the median (IQR).
Table 3. Coagulation variables at baseline, 30, and 60 minutes after IV saline (control) or DDAVP (0.6, 1.2, or 1.8 µg/kg) in anesthetized healthy dogs. Data are presented as the median (IQR).
Table 4. Plasma electrolyte variables at baseline, 30, and 60 minutes after IV saline (Control) or DDAVP (0.6, 1.2, or 1.8 µg/kg) in anesthetized healthy dogs. Data are presented as the median (IQR).
DiscussionIn the present study, desmopressin administration shortened BMBT in anesthetized healthy dogs in a dose-dependent manner. BMBT is a practical clinical test that reflects primary hemostasis at the level of small vessels; therefore, the observed reduction suggests that desmopressin can enhance primary hemostatic function (Brassard and Meyers, 1991; Sato et al., 2000). Although responses varied between dogs, BMBT tended to shorten with increasing dose, indicating a dose-dependent effect on primary hemostasis. Plasma FVIII:Ag increased at 60 minutes after administration, and FVIII:Ag was significantly higher in the 1.8 µg/kg group than in the control group at this time point. In addition, FVIII:Ag increased from baseline to 60 minutes in the 1.2 and 1.8 µg/kg groups. Desmopressin is known to affect FVIII- and vWF-related measures in dogs; however, the association between changes in FVIII:Ag and the observed shortening of BMBT should be interpreted cautiously (Johnstone and Crane, 1986). FVIII:Ag reflects the circulating FVIII protein level rather than FVIII:C (Hoyer, 1981; Chavin, 1984), and primary hemostasis assessed by BMBT is influenced predominantly by platelet–vessel wall interactions (Bowie, 1984; Brassard and Meyers, 1991). Thus, while the increase in FVIII:Ag may be consistent with a systemic hemostatic response to desmopressin, these results do not demonstrate a direct mechanistic link between FVIII:Ag changes and the improvement in BMBT. Further studies incorporating functional assays (e.g., FVIII:C and vWF-related measurements) and evaluating outcomes at multiple time points are warranted to clarify the temporal and mechanistic relationships. The findings have potential clinical relevance for perioperative management in dogs, particularly during major procedures such as open-heart surgery in which bleeding risk can be increased by hemodilution, platelet dysfunction, consumption of coagulation factors, and extracorporeal circulation–related hemostatic disturbances (Bachmann et al., 1975; McKenna et al., 1975; Harker et al., 1980; Bick, 1985). Under such circumstances, an adjunct that improves primary hemostasis could be beneficial. Consistent with this possibility, DDAVP shortened prolonged BMBT in dogs with aspirin-induced platelet dysfunction and in some dogs with chronic liver disease, and was suggested as a hemostatic aid for invasive procedures (Sakai et al., 2003). In addition, a recent case report described uneventful surgical drainage after subcutaneous desmopressin administration in a Doberman Pinscher with type I von Willebrand disease, suggesting possible perioperative utility in selected dogs with hemostatic disorders (Barbry et al., 2021). However, because this was a single case report, the clinical applicability of that observation remains limited. The present results suggest that desmopressin may reduce bleeding tendency, at least as assessed by BMBT, even under general anesthesia. Nevertheless, extrapolation to clinical patients should be made with caution because this study was performed in healthy dogs receiving a single dose under controlled conditions, and BMBT was assessed only at one post-administration time point. Recent canine reports have described perioperative desmopressin use at 1 µg/kg subcutaneously in a dog with type I von Willebrand disease and at 1–3 µg/kg subcutaneously in dogs with mammary carcinoma, although the latter study focused on oncologic outcomes rather than direct hemostatic endpoints (Hermo et al., 2011; Sorenmo et al., 2020; Barbry et al., 2021). In comparison, the present study evaluated single intravenous doses of 0.6–1.8 µg/kg in anesthetized healthy dogs. Because the route of administration, dosing schedule, study population, and study objectives differed substantially among reports, direct dose comparison should be made cautiously. This study has several limitations. First, vWF antigen or activity was not measured; therefore, endothelial release of vWF after desmopressin administration could not be directly assessed (Kaufmann and Vischer, 2003; Olsen et al., 2003). Second, BMBT evaluates primary hemostasis in a standardized mucosal incision model and may not fully reflect bleeding risk in major surgery, where multiple hemostasis components—including coagulation, fibrinolysis, hypothermia, and surgical factors—contribute to clinical hemorrhage (Bucknoff et al., 2014). Third, BMBT was assessed only once at 30 minutes after administration, and no baseline BMBT was obtained; therefore, within-dog comparisons were not possible, and he results may have been influenced by inter-individual variability and local factors such as mucosal perfusion and incision site. Accordingly, the observed differences at 30 minutes should be interpreted as between-group findings at a single post-treatment time point rather than as a direct estimate of within-dog shortening attributable to DDAVP. Thus, the magnitude of the apparent treatment effect should be interpreted cautiously. Fourth, only FVIII:Ag was measured, whereas FVIII:C activity, vWF antigen/activity, and platelet function were not assessed. Because BMBT primarily reflects platelet–vessel wall interactions, the relationship between the increase in FVIII:Ag and the observed BMBT shortening remains indirect. Therefore, these findings should not be overinterpreted as evidence of a specific hemostatic mechanism, and extrapolation to clinical settings should be performed with caution. Fifth, all dogs were studied under a single standardized anesthetic protocol, including medetomidine premedication and isoflurane anesthesia. Because these agents may affect hemodynamics and tissue perfusion, they may have also influenced the BMBT response observed. However, this study was not designed to assess the interactions between DDAVP and specific anesthetic agents. Therefore, the findings should be interpreted within this context. Sixth, blood sampling was performed only at baseline and 30 and 60 minutes after administration, which may not capture earlier peak responses or the full duration of effect. Although no significant electrolyte changes were detected within the 60-minute sampling window, desmopressin-associated water retention and hyponatremia may develop hours after administration. Therefore, delayed electrolyte disturbances cannot be excluded from the present findings, and longer follow-up with serial electrolyte measurements is warranted. Seventh, the sample size in each group was relatively small, and multiple outcome variables were analyzed; thus, we cannot exclude baseline imbalances and chance findings across multiple comparisons. Despite these limitations, the present study provides baseline data indicating that desmopressin may shorten BMBT and increase FVIII:Ag in anesthetized healthy dogs, supporting further investigation of desmopressin in clinical canine surgical patients, including studies incorporating vWF- and FVIII-related functional assays. ConclusionIn healthy dogs, intravenous desmopressin was associated with shorter a dose-dependent shorter BMBT BMBT and increased plasma FVIII:Ag at 60 minutes after administration. Although these changes are consistent with a hemostatic response, this study did not establish a direct mechanistic link between FVIII:Ag and the observed BMBT shortening. Further studies incorporating functional assays (e.g., FVIII:C, vWF antigen/activity, and platelet function testing) and evaluating clinical outcomes in surgical patients are warranted to determine perioperative efficacy, timing, and optimal dosing. Conflict of interestThe authors declare no conflict of interest. FundingNo funding was received for this study. Authors' contributionsShuji Suzuki: conceptualization, study design, data collection, first draft writing, and manuscript editing. Sachiyo Tanaka: study design, data collection, and manuscript editing. Nobuo Kanno: study design, data collection, and manuscript editing. Takuya Yogo: Study design, data collection, and manuscript editing. Yasuji Harada: study design, data collection, and manuscript editing. Yasushi Hara: conceptualization, study design, first draft writing, and manuscript editing. All authors have read and approved the final version of the manuscript. Data availabilityThe data supporting the findings of this study are available from the corresponding author upon reasonable request. ReferencesBachmann, F., McKenna, R., Cole, E.R. and Najafi, H. 1975. The hemostatic mechanism after open-heart surgery. I. Studies on plasma coagulation factors and fibrinolysis in 512 patients after extracorporeal circulation. J. Thorac. Cardiovasc. Surg. 70(1), 76–85; doi:10.1016/S0022-5223(19)40382-6 Barbry, J.B., Poinsard, A.S., Bouzouraa, T., Durand, A. and Balland, O. 2021. Case report of unilateral retrobulbar hematoma associated with von Willebrand disease in a Doberman Pinscher dog. Clin. Case. Rep. 9(3), 1235–1240; doi:10.1002/ccr3.3735 Bick, R.L. 1985. Hemostasis defects associated with cardiac surgery, prosthetic devices, and other extracorporeal circuits. Semin. Thromb. Hemost. 11(3), 249–280; doi:10.1055/s-2007-1004381 Bowie, E.J. 1984. Von Willebrand’s disease: state of the art. Scand. J. Haematol. Suppl. 40, 431–440; doi:10.1111/j.1600-0609.1984.tb02596.x Brassard, J.A. and Meyers, K.M. 1991. Evaluation of the buccal bleeding time and platelet glass bead retention as assays of hemostasis in the dog: the effects of acetylsalicylic acid, warfarin and von Willebrand factor deficiency. Thromb. Haemost. 65(2), 191–195; doi:10.1055/s-0038-1647482 Bucknoff, M.C., Hanel, R.M., Marks, S.L., Motsinger-Reif, A.A. and Suter, S.E. 2014. Evaluation of thromboelastography for prediction of clinical bleeding in thrombocytopenic dogs after total body irradiation and hematopoietic cell transplantation. Am. J. Vet. Res. 75(5), 425–432; doi:10.2460/ajvr.75.5.425 Chavin, S.I. 1984. Factor VIII: structure and function in blood clotting. Am. J. Hematol. 16(3), 297–306; doi:10.1002/ajh.2830160312 Desborough, M.J., Oakland, K., Brierley, C., Bennett, S., Doree, C., Trivella, M., Hopewell, S., Stanworth, S.J. and Estcourt, L.J. 2017. Desmopressin use for minimising perioperative blood transfusion. Cochrane Database Syst. Rev. 7(7), CD001884; doi:10.1002/14651858.CD001884.pub3 Hackmann, T., Gascoyne, R.D., Naiman, S.C., Growe, G.H., Burchill, L.D., Jamieson, W.R.E., Sheps, S.B., Schechter, M.T. and Townsend, G.E. 1989. A trial of desmopressin (1-desamino-8-D-arginine vasopressin) to reduce blood loss in uncomplicated cardiac surgery. N. Engl. J. Med. 321(21), 1437–1443; doi:10.1056/NEJM198911233212104 Harker, L.A., Malpass, T.W., Branson, H.E., Hessel, E.A. and Slichter, S.J. 1980. Mechanism of abnormal bleeding in patients undergoing cardiopulmonary bypass: acquired transient platelet dysfunction associated with selective alpha-granule release. Blood 56(5), 824–834; doi:10.1182/blood.V56.5.824.824 Hermo, G.A., Turic, E., Angelico, D., Scursoni, A.M., Gomez, D.E., Gobello, C. and Alonso, D.F. 2011. Effect of adjuvant perioperative desmopressin in locally advanced canine mammary carcinoma and its relation to histologic grade. J. Am. Anim. Hosp. Assoc. 47(1), 21–27; doi:10.5326/JAAHA-MS-5509 Hoyer, L. 1981. The factor VIII complex: structure and function. Blood 58(1), 1–13; doi:10.1182/blood.V58.1.1.1 Johnstone, I.B. and Crane, S. 1986. The effects of desmopressin on hemostatic parameters in the normal dog. Can. J. Vet. Res. 50(2), 265–271. Kaufmann, J.E. and Vischer, U.M. 2003. Cellular mechanisms of the hemostatic effects of desmopressin (DDAVP). J. Thromb. Haemost. 1(4), 682–689; doi:10.1046/j.1538-7836.2003.00190.x McKenna, R., Bachmann, F., Whittaker, B., Gilson, J.R. and Weinberg, M. 1975. The hemostatic mechanism after open-heart surgery. II. Frequency of abnormal platelet functions during and after extracorporeal circulation. J. Thorac. Cardiovasc. Surg. 70(2), 298–308; doi:10.1016/S0022-5223(19)40355-3 Olsen, E.H.N., Mccain, A.S., Merricks, E.P., Fischer, T.H., Dillon, I.M., Raymer, R.A., Bellinger, D.A., Fahs, S.A., Montgomery, R.R., Keith, J.C., Schaub, R.G. and Nichols, T.C. 2003. Comparative response of plasma VWF in dogs to up-regulation of VWF mRNA by interleukin-11 versus Weibel-Palade body release by desmopressin (DDAVP). Blood 102(2), 436–441; doi:10.1182/blood-2003-01-0290 Picchio, M., Marcucci, C., Jaques, C., Mauron, S. and Zuercher, M. 2025. Efficacy and safety of desmopressin in terms of bleeding and transfusion in cardiac surgery with cardiopulmonary bypass: a systematic review and meta-analysis. Heart. Lung. Circ. 34(7), 674–692; doi:10.1016/j.hlc.2025.01.003 Sakai, M., Watari, T., Miura, T., Maruyama, H., Koie, H., Yamaya, Y., Takeuchi, A. and Hasegawa, A. 2003. Effects of DDAVP administrated subcutaneously in dogs with aspirin-induced platelet dysfunction and hemostatic impairment due to chronic liver diseases. J. Vet. Med. Sci. 65(1), 83–86; doi:10.1292/jvms.65.83 Salzman, E.W., Weinstein, M.J., Weintraub, R.M., Ware, J.A., Thurer, R.L., Robertson, L., Donovan, A., Gaffney, T., Bertele, V., Troll, J., Smith, M. and Chute, L.E. 1986. Treatment with desmopressin acetate to reduce blood loss after cardiac surgery. A double-blind randomized trial. N. Engl. J. Med. 314(22), 1402–1406; doi:10.1056/NEJM198605293142202 Sato, I., Anderson, G.A. and Parry, B.W. 2000. An interobserver and intraobserver study of buccal mucosal bleeding time in Greyhounds. Res. Vet. Sci. 68(1), 41–45; doi:10.1053/rvsc.1999.0334 Sorenmo, K., Durham, A.C., Evans, B., Scavello, H. and Stefanovski, D. 2020. A prospective randomized trial of desmopressin in canine mammary carcinoma. Vet. Comp. Oncol. 18(4), 796–803; doi:10.1111/vco.12619 Umlas, J. 1976. Fibrinolysis and disseminated intravascular coagulation in open heart surgery. Transfusion 16(5), 460–463; doi:10.1046/j.1537-2995.1976.16577039303.x | ||
| How to Cite this Article |
| Pubmed Style Suzuki S, Tanaka S, Kanno N, Yogo T, Harada Y, Hara Y. Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Vet. J.. 2026; 16(5): 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 Web Style Suzuki S, Tanaka S, Kanno N, Yogo T, Harada Y, Hara Y. Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. https://www.openveterinaryjournal.com/?mno=308943 [Access: June 26, 2026]. doi:10.5455/OVJ.2026.v16.i5.4 AMA (American Medical Association) Style Suzuki S, Tanaka S, Kanno N, Yogo T, Harada Y, Hara Y. Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Vet. J.. 2026; 16(5): 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 Vancouver/ICMJE Style Suzuki S, Tanaka S, Kanno N, Yogo T, Harada Y, Hara Y. Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Vet. J.. (2026), [cited June 26, 2026]; 16(5): 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 Harvard Style Suzuki, S., Tanaka, . S., Kanno, . N., Yogo, . T., Harada, . Y. & Hara, . Y. (2026) Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Vet. J., 16 (5), 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 Turabian Style Suzuki, Shuji, Sachiyo Tanaka, Nobuo Kanno, Takuya Yogo, Yasuji Harada, and Yasushi Hara. 2026. Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Veterinary Journal, 16 (5), 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 Chicago Style Suzuki, Shuji, Sachiyo Tanaka, Nobuo Kanno, Takuya Yogo, Yasuji Harada, and Yasushi Hara. "Effect of desmopressin on buccal mucosal bleeding time in healthy dogs." Open Veterinary Journal 16 (2026), 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 MLA (The Modern Language Association) Style Suzuki, Shuji, Sachiyo Tanaka, Nobuo Kanno, Takuya Yogo, Yasuji Harada, and Yasushi Hara. "Effect of desmopressin on buccal mucosal bleeding time in healthy dogs." Open Veterinary Journal 16.5 (2026), 2610-2618. Print. doi:10.5455/OVJ.2026.v16.i5.4 APA (American Psychological Association) Style Suzuki, S., Tanaka, . S., Kanno, . N., Yogo, . T., Harada, . Y. & Hara, . Y. (2026) Effect of desmopressin on buccal mucosal bleeding time in healthy dogs. Open Veterinary Journal, 16 (5), 2610-2618. doi:10.5455/OVJ.2026.v16.i5.4 |

