




| Short Communication | ||
Open Vet. J.. 2026; 16(5): 3247-3254 Open Veterinary Journal, (2026), Vol. 16(5): 3247-3254 Short Communication Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failureTung Hsueh1, I-Ping Chan1*, Chung-Chun Yang1 and Shiun-Long Lin1,21Veterinary Medical Teaching Hospital, National Chung Hsing University, Taichung City, Taiwan 2Department of Veterinary Medicine, National Chung Hsing University, Taichung City, Taiwan *Corresponding Author: I-Ping Chan. Veterinary Medical Teaching Hospital, National Chung Hsing University, Taichung City, Taiwan. Email: cutejamie.tw [at] gmail.com Submitted: 23/10/2025 Revised: 03/03/2026 Accepted: 14/03/2026 Published: 31/05/2026 © 2025 Open Veterinary Journal
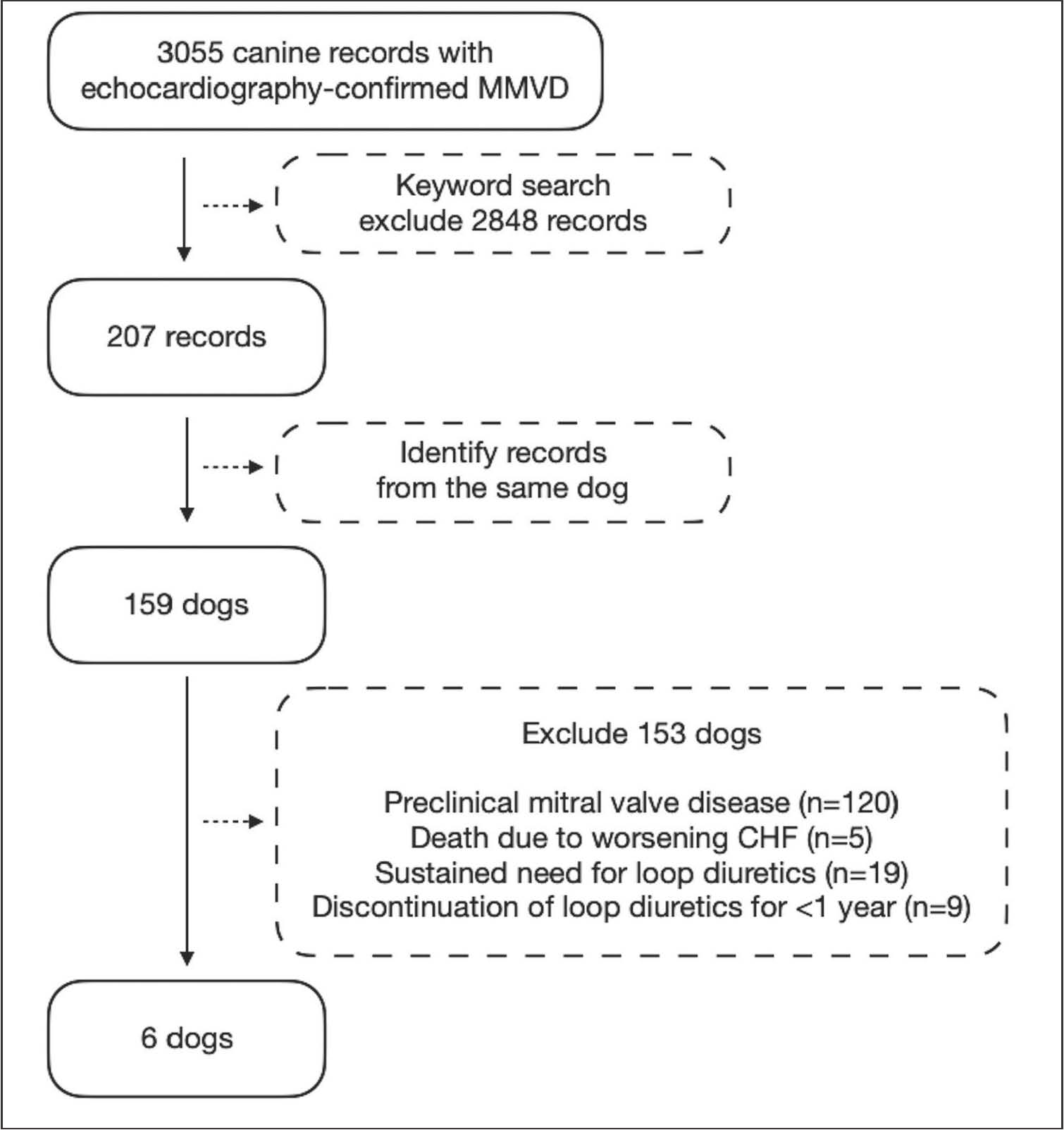
ABSTRACTBackground: Myxomatous mitral valve disease (MMVD) is a common cause of congestive heart failure (CHF) in small-breed dogs. Clinical observations suggest that discontinuation of loop diuretics may be feasible in a subset of dogs with MMVD and CHF. Aim: To characterize dogs with MMVD-related CHF that achieved stability following loop diuretic withdrawal and to investigate potential contributing factors. Methods: We retrospectively analyzed 3,055 canine medical records of dogs diagnosed with MMVD (2012–2022) from the National Chung Hsing University Veterinary Medical Teaching Hospital database. Dogs considered stable and not requiring diuretic administration for at least 1 year after CHF diagnosis were included. Results: Six dogs (5 Maltese and 1 Toy Poodle) with a median age of 8.5 years and a median weight of 3.18 kg met the inclusion criteria. These dogs achieved stability after a median treatment duration of 675 days (range: 77–917 days) and were followed up for a period of 386–1,572 days. The presence of azotemia, radiographic evidence of reduced heart size, and evidence of long-term clinical stability supported diuretic tapering. All cardiac medications were discontinued in three dogs, while the remaining three continued pimobendan-based therapy. Conclusion: CHF secondary to MMVD in dogs can stabilize in rare instances without lifelong diuretic administration. These observations suggest that reversible or transient factors may contribute to the initial presentation of CHF in selected cases. Regular cardiac and renal assessments may help in identifying suitable candidates for diuretic adjustment when concurrent systemic conditions, such as azotemia, pose a limiting side effect despite sustained clinical stability or in rare instances of prolonged clinical stability without CHF signs. This approach facilitates individualized CHF management and improves the quality of life of both pets and their owners. Keywords: Discontinue, Furosemide, Long-term follow-up, Pulmonary edema. IntroductionMyxomatous mitral valve disease (MMVD) is a prevalent cardiac condition in older, small-to-medium breed dogs, particularly in Cavalier King Charles Spaniels, Dachshunds, Miniature Poodles, and Toy Poodles. In North America, cardiac disease affects 10% of dogs presenting to general veterinary practices, with MMVD accounting for 75% of these cases (Keene et al., 2019; O'Brien et al., 2021). A retrospective cohort study conducted in England reported an MMVD prevalence of 0.36% (Mattin et al., 2015). The 2019 American College of Veterinary Internal Medicine guidelines advocate for MMVD treatment based on disease staging, which necessitates auscultation, thoracic radiography, and echocardiography. The cornerstone treatments for congestive heart failure (CHF) include diuretics, inodilators, renin-angiotensin-aldosterone system inhibitors, and vasodilators. Loop diuretics are key in managing CHF by reducing intravascular volume and mitigating congestion signs, such as pulmonary edema and pleural effusion (Keene et al., 2019). Lifelong medication, particularly loop diuretics, is commonly required in dogs that develop CHF, given the progressive nature of MMVD. With appropriate medical management, the expected survival time after CHF diagnosis ranges from 6 to 33 months (Borgarelli et al., 2008; Borgarelli and Haggstrom, 2010). In rare instances with specific clinical indications, such as azotemia or sustained clinical stability, CHF may stabilize sufficiently to allow for cautious tapering of loop diuretics without recurrence, as reported in two Chihuahuas (Wesselowski, 2023). Serial cardiac evaluations revealed reversed left-sided cardiac remodeling and reduced mitral regurgitation, enabling furosemide discontinuation in both Chihuahuas, which had been previously diagnosed with CHF secondary to severe mitral regurgitation resulting from a flail anterior mitral valve leaflet. Based on our clinical observations, this unique stability has also been noted in several dogs with MMVD and CHF. These cases suggest that long-term stability is not exclusively limited to dogs initially diagnosed with chordae tendineae rupture, implying that other factors may contribute to transient episodes of heart failure in dogs without lifelong medication. In this article, we describe these cases and explore the factors that contribute to their unique stability. Materials and MethodsWe retrospectively reviewed medical records from October 2012 to December 2022 at the Veterinary Medical Teaching Hospital of National Chung Hsing University. A total of 3,055 canine records with MMVD confirmed by echocardiography were identified, excluding cases with congenital or other acquired heart diseases. A keyword search using terms such as "taper," "stop," "discontinue," and "resolve" yielded 207 records describing 159 dogs. Following a detailed review, we excluded dogs with preclinical mitral valve disease (n=120), cardiac-related death due to worsening CHF (n=5), sustained need for loop diuretics (n=19), or discontinuation of loop diuretics for less than 1 year without CHF relapse (n=9) were excluded, as sustained clinical stability was defined by the ability to maintain complete diuretic withdrawal for ≥1 year. This resulted in six dogs being included in the study. The case screening process is illustrated in Figure 1.
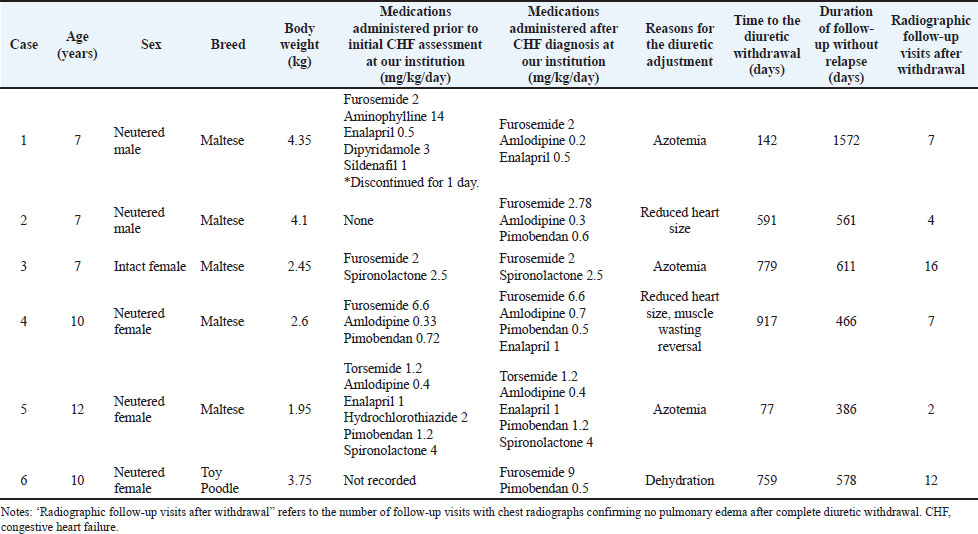
Fig. 1. Flow chart of the case screening process. Ethical approvalEthical approval was not required due to the retrospective and observational design of the study. As part of the standard registration process at our teaching hospital, clients are informed that their medical data may be used for research and teaching purposes. Consent is implied by the registration. Results and DiscussionSix dogs diagnosed with MMVD were included in this study. These dogs remained clinically stable without diuretic intervention for at least 1 year following CHF diagnosis and subsequent CHF treatment. The cohort consisted of five Maltese and one Toy Poodle, with a median age of 8.5 years (range: 7–12 years) and a median body weight of 3.18 kg (range: 1.95–4.35). Case 1 was referred because of worsening tachypnea 1 day after discontinuing a 1-month course of loop diuretics for managing CHF. Case 2, with preclinical MMVD and monitored for 609 days at our institution, presented with increased coughing and an elevated sleeping respiratory rate for 3 days before the visit. Cases 3 and 4 were referred by their family veterinarians, who had initially diagnosed and treated their CHF signs. Case 5 was referred for a second opinion after experiencing acute respiratory distress during a family camping trip, which prompted early termination of the trip and a diagnosis of MMVD-related pulmonary edema at a referring hospital the following day. Case 6 presented with tachypnea and nocturnal coughing and was hospitalized in our internal medicine department for 1 day to stabilize pulmonary edema. Upon presentation, a left apical systolic heart murmur was detected in all cases, with an intensity ranging from grade III (case 3) to grade V with a palpable thrill (remaining cases). Cases 1 and 6 were classified as grade IV. Thoracic radiographs were obtained as part of a routine clinical evaluation, including at least one dorsoventral or ventrodorsal view and one lateral view. Attention was given to appropriate positioning and image acquisition during maximal inspiration whenever possible. The radiographic interpretation included the assessment of the cardiac silhouette size, pulmonary parenchymal patterns, and pulmonary vasculature. Thoracic radiographs revealed vertebral heart sizes ranging from 9.3 to 12.8. Pulmonary edema, characterized by interstitial-to-alveolar lung patterns, was confirmed in three patients (cases 1, 2, and 6) at presentation, suggesting CHF (Diana et al., 2009). The remaining three cases (cases 3, 4, and 5) exhibited no pulmonary edema on initial radiographs. Medical records and referral information indicated that these dogs had previously presented to referring clinics for tachypnea or respiratory distress, where pulmonary edema was reportedly confirmed radiographically. Clinical signs and radiographic abnormalities reportedly improved prior to referral following diuretic therapy at those institutions. All three cases had a documented history of respiratory distress responsive to diuretic therapy, consistent with previous episodes of CHF. Nevertheless, the absence of documented pulmonary edema at our hospital at the time of presentation in three cases introduces potential heterogeneity in the presentation and stage of CHF. Consequently, the diagnosis of CHF in these cases, based on a combination of referral history and treatment response, warrants cautious interpretation due to the retrospective design of the study. MMVD was confirmed in all cases based on echocardiographic findings of thickened mitral valve leaflets and subsequent mitral regurgitation. Echocardiographic examinations were performed by experienced cardiologists or under their direct supervision. Standard right and left parasternal long- and short-axis views were routinely acquired. Assessments included valvular morphology and motion, ventricular systolic and diastolic function, and blood flow dynamics. These evaluations constituted a comprehensive cardiac assessment uniformly applied to all cases undergoing echocardiography. Table 1 summarizes the descriptive data and medication information for each case. Although cases 3 and 4 required repeated diuretic dose adjustments due to recurrent pulmonary edema (Fig. 2), all six dogs ultimately achieved clinical stability, defined as the absence of pulmonary edema on radiographs and clinical signs of CHF during follow-up. Subsequently, the dogs underwent successful tapering and complete withdrawal of loop diuretics without relapse for ≥1 year (Table 1). In addition to clinical stability, factors supporting diuretic dose reduction included azotemia (cases 1, 3, and 5), a reduction in heart size compared with measurements at the time of CHF (cases 2, 3, 4, and 5), and dehydration detected on physical examination (case 6). Improvement in muscle condition score, as assessed using the muscle condition scoring system from the World Small Animal Veterinary Association (Freeman et al., 2011), was documented during follow-up in case 4. This finding is a supportive indicator of overall clinical improvement (Ineson et al., 2019). Table 1. Signalment, initial diuretic dosages, and timeline of each case.
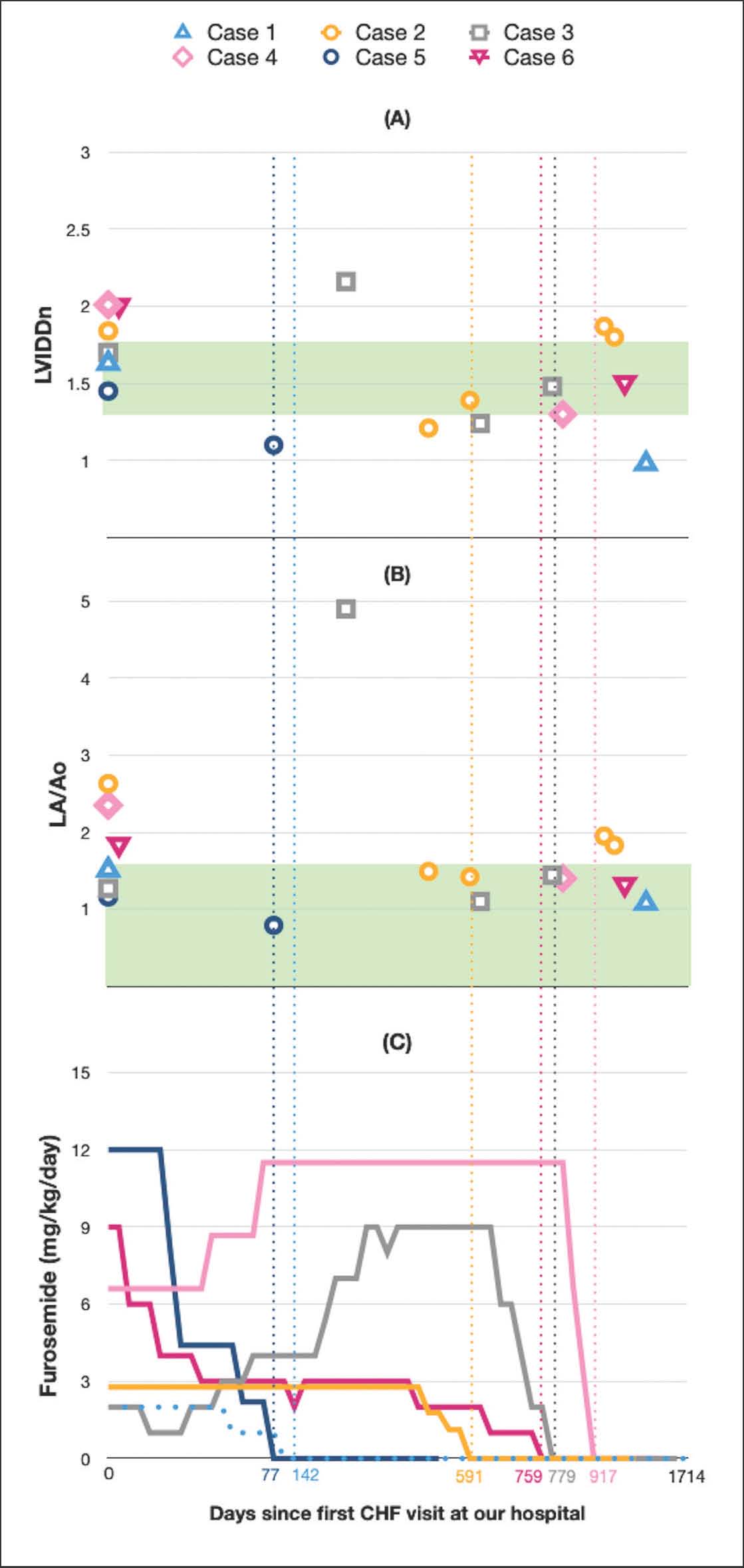
Fig. 2. Temporal changes in (A) normalized left ventricular internal diameter in diastole (LVIDDn, measured via M-mode in the right parasternal short-axis view at the papillary muscle level), (B) left atrial-to-aortic root ratio (LA/Ao, measured using the 2D method, obtained at early diastole (immediately after aortic valve closure) in the right parasternal short-axis view at the heart base), and (C) loop diuretic dosage in six cases. Each case is represented by a unique mark and color (see legends at the top of the figure). The X-axis represents time and is shared across the panels. Day 0 on the X-axis represents the first CHF visit to our hospital for each case. The vertical dashed lines indicate the time of complete diuretic withdrawal for each case, and the exact days from the first CHF visit to diuretic withdrawal are shown on the X-axis using the corresponding case-specific colors. The value “1,714” indicates the longest follow-up duration observed in case 1. The green shaded areas denote the reference ranges. Overall, this figure illustrates the longitudinal changes in cardiac size echocardiographic indices in relation to diuretic dosage adjustments, visualizing the timing of serial echocardiographic evaluations and the point of complete diuretic withdrawal during long-term follow-up. The median time from the first presentation for CHF to complete discontinuation of loop diuretics was 675 days (range: 77–917), with a median follow-up duration of 569.5 days (range: 386–1,572) after withdrawal. During the follow-up period, two cases developed neoplasms: a perianal tumor in case 2 and a mammary gland tumor in case 3. Both cases were successfully treated surgically at 308 and 391 days after loop diuretic withdrawal, respectively. Case 4 was diagnosed with a paroxysmal movement disorder, which was well controlled at 483 days after the initial presentation. Case 6 developed ataxia and limb stiffness, raising suspicion of Cushing’s disease with endocrine-related myopathy, 405 days after furosemide withdrawal. No systemic diseases were identified in cases 1 and 5. Cardiac medications were completely discontinued in three cases (cases 1, 3, and 5). The remaining three cases continued pimobendan therapy, with case 4 additionally receiving amlodipine and spironolactone, and case 6 continuing enalapril therapy at the end of follow-up. Table 1 summarizes the clinical timelines for each case. Fig. 2 illustrates the longitudinal changes in echocardiographic indices of cardiac size and loop diuretic dosage over time in the six cases, with the timing of complete diuretic withdrawal indicated. Among 3,055 echocardiographic reports indicating a diagnosis of MMVD over a 10-year period, only six dogs met the criteria for sustained loop diuretic discontinuation. Although the absolute patient-level prevalence could not be determined, these findings represent a small fraction of the clinical population, underscoring their exceptional nature. The definitive reason for the alleviation of CHF in these six dogs remains unknown. A recent case report described CHF resolution in two Chihuahuas secondary to mitral valve disease without surgical intervention (Wesselowski, 2023). Both Chihuahuas had ruptured chordae tendineae of the anterior mitral valve leaflet, resulting in CHF that resolved after furosemide was discontinued after 4 and 18 months. Among the six dogs included in our study, only case 1 had an echocardiographic record of a flail mitral valve leaflet. This case shares notable similarities with two previously reported Chihuahuas that exhibited CHF resolution and reverse remodeling following acute decompensation associated with flail mitral valve leaflets. Case 1 also demonstrated a subsequent reduction in cardiac dimensions and absence of an audible heart murmur at his last echocardiographic examination (1,070 days after loop diuretic discontinuation). Although echocardiography was not performed at the time of initiating diuretic tapering, it is reasonable to speculate that echocardiographic findings at that stage, if available, might have resembled those described in the reported Chihuahuas, including decreased left atrial size, reduced left ventricular internal dimensions, and attenuation of mitral regurgitation severity. Such changes would be consistent with partial reverse remodeling, potentially related to chordae tendineae rupture or transient hemodynamic decompensation with subsequent myocardial compensation. It should also be noted that 2D echocardiography may not reliably detect all chordae tendineae ruptures; therefore, additional cases in this series may have had undetected structural lesions contributing to CHF presentation and subsequent remission. In case 5, echocardiography confirmed MMVD, and aggressive diuretic therapy stabilized the clinical signs. Primary respiratory disease was ruled out, and the heart size remained within the normal range throughout the follow-up period (Fig. 2), a finding that was occasionally observed in dogs with acute CHF. Situational or stress-related factors, such as the recent camping trip, may have contributed to the onset or exacerbation of respiratory symptoms. However, the marked clinical response to diuretic therapy, the absence of primary respiratory abnormalities, and a markedly elevated NT-proBNP concentration at initial presentation (2,118.2 pmol/l; IDEXX reference laboratory) support CHF as the primary cause of the initial respiratory distress. In this context, although a definitive causal relationship cannot be established, stress-related mechanisms may have contributed to the observed acute hemodynamic burden. Neurohormonal modulation, including sympathetic activation and transient increases in afterload and myocardial oxygen demand, has been proposed as a potential pathway linking emotional or situational stress to acute CHF decompensation in susceptible individuals (Nalivaiko, 2011; Silva and Fontes, 2019). Similar stress-induced cardiopulmonary decompensation has been described in human patients, where emotional stress may precipitate transient heart failure through catecholamine-mediated mechanisms, even in the absence of structural progression (Omerovic and Redfors, 2025). Stress-related transient CHF has been reported in cats (Novo Matos et al., 2018). These mechanisms may result in reversible cardiac dysfunction under specific conditions. However, this phenomenon remains poorly characterized in dogs with MMVD, and its exact pathophysiology is unclear. To explore this hypothesis, further investigations with larger sample sizes are warranted. The specific factors contributing to the resolution of CHF in the remaining four cases were not identified. Interestingly, these four cases were subsequently found to have other systemic diseases during the follow-up period. Whether these diseases influenced CHF improvement or were coincidental remains unclear. This observation suggests that systemic health may warrant further investigation to understand its potential role in the outcomes of CHF. The six cases in our study suggest that CHF in dogs with MMVD may stabilize to a point where diuretic therapy is no longer required in rare instances. Importantly, any diuretic adjustment or reduction was considered only in the context of sustained clinical stability. Regular cardiac and renal assessments may help identify dogs in which diuretic dose reduction is considered because azotemia or dehydration becomes a limiting side effect of diuretic therapy, while CHF remains clinically controlled. Thorough monitoring of concurrent systemic conditions, including renal parameters, may help minimize long-term diuretic-related adverse effects and improve the quality of life for both pets and owners. This study has several inherent limitations related to its retrospective design. Clinical management was not protocol-driven; therefore, the attending veterinarian determined the timing of echocardiographic examinations, drug combinations, and the rate of diuretic tapering based on clinical judgment and owner compliance, rather than standardized criteria. Consequently, in some cases (cases 1, 3, and 5), echocardiographic assessment was performed only after pharmacologic therapy had been initiated to stabilize clinical signs, precluding the exclusion of potential drug effects on cardiac measurements. Furthermore, not every diuretic dose adjustment was accompanied by echocardiographic reassessment, which limits the mechanistic interpretation of temporal changes in cardiac size. In addition, the cardiac biomarker NT-proBNP has demonstrated diagnostic and prognostic value in dogs with MMVD (Chanmongkolpanit et al., 2024; Iwasa et al., 2025). However, NT-proBNP measurement was available only for case 5 at the initial presentation of CHF because most cases were enrolled before NT-proBNP testing was routinely implemented at our institution. Consequently, the evaluation of serial NT-proBNP across all cases was not feasible for comparative analysis. Furthermore, the limited sample size and the lack of a control group of dogs requiring lifelong diuretic therapy constrain the generalizability of our findings and preclude the identification of predictors for successful diuretic withdrawal. A further limitation of this study is the use of a keyword-based search strategy to identify cases of loop diuretic tapering or discontinuation. This approach may have failed to capture relevant cases if medication adjustments were not explicitly documented using the pre-selected keywords, potentially introducing selection bias. However, this methodology was deemed a pragmatic approach for identifying potential cases within a large retrospective database, considering the retrospective study design and the infrequent nature of the clinical phenomenon under investigation. Future prospective studies employing larger, standardized datasets are warranted to elucidate the underlying mechanisms and to explore the potential criteria for safe diuretic withdrawal in select cases. Further investigation into the frequency and reversibility of stress-related CHF, as well as potential predictors, may also yield additional insights into MMVD management. AcknowledgmentsWe are grateful to ANIWARE Co., Ltd., for providing financial assistance with the English editing of the manuscript. Conflict of interestThe authors declare no conflict of interest. FundingThis study received no specific grant. Authors' contributionsTung Hsueh: data collection, analysis, and writing of the original draft. I.-Ping Chan: concept and design, writing, review, and editing. Chung-Chun Yang: Data collection. Shiun-Long Lin: Supervision Data availabilityThe data that support the findings of this study are not openly available due to sensitivity reasons and are available from the corresponding author upon reasonable request. ReferencesBorgarelli, M. and Haggstrom, J. 2010. Canine degenerative myxomatous mitral valve disease: natural history, clinical presentation and therapy. Vet. Clin. North. Am. Small. Anim. Pract. 40(5), 651–663. Borgarelli, M., Savarino, P., Crosara, S., Santilli, R.A., Chiavegato, D., Poggi, M., Bellino, C., La Rosa, G., Zanatta, R., Haggstrom, J. and Tarducci, A. 2008. Survival characteristics and prognostic variables of dogs with mitral regurgitation attributable to myxomatous valve disease. J. Vet. Intern. Med. 22(1), 120–128. Chanmongkolpanit, K., Riengvirodkij, N., Channgam, P., Kaenchan, P., Buayam, W., Janhirun, Y., Phonarknguen, R., Tansakul, M. and Sakcamduang, W. 2024. How accurate are NT-proBNP, ANP, and cTnI levels in diagnosing dogs with myxomatous mitral valve disease?. Open Vet. J. 14(6), 1426–1441. Diana, A., Guglielmini, C., Pivetta, M., Sanacore, A., Di Loria, A. and Cipone, M. 2009. Radiographic features of cardiogenic pulmonary edema in dogs with mitral regurgitation: 61 cases (1998–2007). J. Am. Vet. Med. Assoc. 235(9), 1058–1063. Freeman, L., Becvarova, I., Cave, N., Mackay, C., Nguyen, P., Rama, B., Takashima, G., Tiffin, R., Tsjimoto, H. and Van Beukelen, P. 2011. WSAVA nutritional assessment guidelines. J. Small. Anim. Pract. 52(7), 385–396. Ineson, D.L., Freeman, L.M. and Rush, J.E. 2019. Clinical and laboratory findings and survival time associated with cardiac cachexia in dogs with congestive heart failure. J. Vet. Intern. Med. 33(5), 1902–1908. Iwasa, N., Kumazawa, R., Shimizu, M., Okamoto, T., Kawabe, M., Iwata, M., Watanabe, K., Kobatake, Y., Takashima, S. and Nishii, N. 2025. Prognostic value of circulating cardiac and renal biomarkers in dogs with myxomatous mitral valve disease. Res. Vet. Sci. 189, 105649. Keene, B.W., Atkins, C.E., Bonagura, J.D., Fox, P.R., Häggström, J., Fuentes, V.L., Oyama, M.A., Rush, J.E., Stepien, R. and Uechi, M. 2019. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 33(3), 1127–1140. Mattin, M.J., Boswood, A., Church, D.B., Mcgreevy, P.D., O’Neill, D.G., Thomson, P.C. and Brodbelt, D.C. 2015. Degenerative mitral valve disease: survival of dogs attending primary-care practice in England. Prev. Vet. Med. 122(4), 436–442. Nalivaiko, E. 2011. Animal models of psychogenic cardiovascular disorders: what we can learn from them and what we cannot. Clin. Exp. Pharmacol. Physiol. 38(2), 115–125. Novo Matos, J., Pereira, N., Glaus, T., Wilkie, L., Borgeat, K., Loureiro, J., Silva, J., Law, V., Kranjc, A., Connolly, D.J. and Luis Fuentes, V. 2018. Transient myocardial thickening in cats associated with heart failure. J. Vet. Intern. Med. 32(1), 48–56. O’Brien, M.J., Beijerink, N.J. and Wade, C.M. 2021. Genetics of canine myxomatous mitral valve disease. Anim. Genet. 52(4), 409–421. Omerovic, E. and Redfors, B. 2025. Takotsubo syndrome: pathophysiological insights and innovations in patient care. Nat. Rev. Cardiol; doi: 10.1038/s41569-025-01211-5 Silva, C.C. and Fontes, M.A.P. 2019. Cardiovascular reactivity to emotional stress: the hidden challenge for pets in the urbanized environment. Physiol. Behav. 207, 151–158. Wesselowski, S. 2023. Resolution of congestive heart failure and reverse remodeling in two Chihuahuas with flail mitral valve leaflets. J. Vet. Cardiol. 47, 55–63. | ||
| How to Cite this Article |
| Pubmed Style Hsueh T, Chan I, Yang C, Lin S. Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Vet. J.. 2026; 16(5): 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 Web Style Hsueh T, Chan I, Yang C, Lin S. Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. https://www.openveterinaryjournal.com/?mno=292213 [Access: June 26, 2026]. doi:10.5455/OVJ.2026.v16.i5.64 AMA (American Medical Association) Style Hsueh T, Chan I, Yang C, Lin S. Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Vet. J.. 2026; 16(5): 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 Vancouver/ICMJE Style Hsueh T, Chan I, Yang C, Lin S. Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Vet. J.. (2026), [cited June 26, 2026]; 16(5): 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 Harvard Style Hsueh, T., Chan, . I., Yang, . C. & Lin, . S. (2026) Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Vet. J., 16 (5), 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 Turabian Style Hsueh, Tung, I-ping Chan, Chung-chun Yang, and Shiun-long Lin. 2026. Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Veterinary Journal, 16 (5), 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 Chicago Style Hsueh, Tung, I-ping Chan, Chung-chun Yang, and Shiun-long Lin. "Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure." Open Veterinary Journal 16 (2026), 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 MLA (The Modern Language Association) Style Hsueh, Tung, I-ping Chan, Chung-chun Yang, and Shiun-long Lin. "Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure." Open Veterinary Journal 16.5 (2026), 3247-3254. Print. doi:10.5455/OVJ.2026.v16.i5.64 APA (American Psychological Association) Style Hsueh, T., Chan, . I., Yang, . C. & Lin, . S. (2026) Rare stability in dogs with myxomatous mitral valve disease: Clinical observations of loop diuretic withdrawal after congestive heart failure. Open Veterinary Journal, 16 (5), 3247-3254. doi:10.5455/OVJ.2026.v16.i5.64 |

